
Public health and the
food and drinks industry:
The governance and ethics
of interaction
Lessons from research, policy and practice
FUNDERS
GOVERNMENT
NON-
GOVERNMENTAL
ORGANISATIONS
CIVIL SOCIETY
ORGANISATIONS
POLICY-
MAKERS
RESEARCHERS
FOOD AND DRINKS
INDUSTRY
?

ISBN E-version: 978-1-874279-16-7
Produced by the UK Health Forum.
Funded by the Canadian Institutes of Health Research (CIHR) – Institute of Population and Public Health (IPPH) and
the International Development Research Centre (IDRC), with contributions in kind from the UK Health Forum (UKHF).
The views expressed in this paper are those of the authors and do not necessarily reflect those of UKHF, IDRC, CIHR or
the Government of Canada.
Editor: Modi Mwatsama.
© UK Health Forum 2018
About the UK Health Forum
UK Health Forum
Fleetbank House
2-6 Salisbury Square
London EC4Y 8JX
www.ukhealthforum.org.uk
The UK Health Forum is a charitable alliance of professional and public interest organisations working to reduce the
risk of avoidable non-communicable diseases by developing evidence-based public health policy and supporting its
implementation through advocacy and information provision.
Public health and the food and drinks industry: The governance and ethics of
interaction. Lessons from research, policy and practice
Acknowledgements
This piece of work was informed in part through dialogue at the workshop
Improving governance for better health:
Strengthening the governance of diet and nutrition partnerships for the prevention of chronic diseases
, held at the
Rockefeller Foundation Bellagio Center, Italy, from 26 to 30 October 2015.
The UK Health Forum would like to thank the anonymous peer reviewers who reviewed the submissions, and also the
members of the Project Advisory Group (listed on the next page) who provided valuable oversight to the project.
Additional editing by Wordworks.
Design by Sally Geeve.
How to cite this document
UK Health Forum (2018). Public health and the food and drinks industry: The governance and ethics of interaction.
Lessons from research, policy and practice. London: UKHF.

Project Advisory Group
Professor Rima Afifi, American University of Beirut and University of Iowa (since September 2017).
Renaud F Boulanger, International Development Research Centre (until September 2016)
Professor Jeff Collin, University of Edinburgh
Dr Erica Di Ruggiero, Dalla Lana School of Public Health, University of Toronto.
Dr Fabio Gomes, Pan American Health Organization
Greg Hallen, International Development Research Centre
Dr Zee Leung, International Development Research Centre
Dr Modi Mwatsama, UK Health Forum
Declarations of interests
Professor Rima Afifi
None delcared.
Renaud F Boulanger
None declared.
Professor Jeff Collin
None declared.
Dr Erica Di Ruggiero
None declared.
Dr Fabio Gomes
None declared.
Greg Hallen
None declared.
Dr Zee Leung
None declared.
Dr Modi Mwatsama
Brother is a pricing analyst for Dunnhumby, a subsidiary of the UK retailer Tesco. Brother’s work does not influence my
day-to-day work.

conflict of interest
Ensemble Prévenons l’Obésité Des Enfants / Together Let’s Prevent Childhood Obesity
Frente pela Regulação da Relação Público Privado em Alimentação e Nutrição (Front for
Regulation of the Public-Private Relationship in Food and Nutrition), Brazil
Global Burden of Disease
Guideline Daily Amount
Global Health Council
Healthy Caribbean Coalition
High-Level Meeting
International Life Sciences Institute
Instituto de Nutrición y Tecnología de los Alimentos
(Institute of Nutrition and Food Technology), Chile
non-communicable disease
non-governmental organisation
Observatorio Mexicano de Enfermedades No Transmisibles
(Mexican Observatory on Noncommunicable Diseases)
sugar-sweetened beverages
United Nations
United Nations High-Level Meeting
World Health Organization
Acronyms
COI
EPODE
FRRPPAN
GBD
GDA
GHC
HCC
HLM
ILSI
INTA
NCD
NGO
OMENT
SSBs
UN
UN HLM
WHO

5
Foreword
Dr Francesco Branca
Introduction
Erica Di Ruggiero, Greg Hallen, Zee Leung and Modi Mwatsama
CASE 1 The development of a national obesity and diabetes prevention and
control strategy in Mexico: actors, actions and conflicts of interest
Simón Barquera, Karina Sánchez-Bazán, Angela Carriedo and Boyd Swinburn
CASE 2 Conflicting goals and weakened actions: lessons learned from the
political process of increasing sugar-sweetened beverage taxation in Chile
Cristóbal Cuadrado, María Teresa Valenzuela and Sebastián Peña
CASE 3 Sugar-sweetened beverages, non-communicable diseases and the limits
of self-regulation in Fiji
Neil Sharma and Melissa Mialon
CASE 4 Political action by researchers, professionals, activists and policy-makers
to advance the food and nutrition regulatory agenda in Brazil
Inês Rugani Ribeiro de Castro, Camila Paes de Carvalho, Paulo Castro Jr, Luciene Burlandy,
Veruska Alexandre, Ana Feldenheimer da Silva, Luciana Maldonado and Daniela Canella
CASE 5 Industry involvement in government nutrition advisory groups in
Canada: a decade of inaction on trans fat and sodium
Bill Jeery
CASE 6 Food industry permeating public institutions: the case of the Chilean
Institute of Nutrition and Food Technology
Sebastián Peña, Cecilia Castillo, Cristóbal Cuadrado and María Teresa Valenzuela
CASE 7 Participation of non-state actors in developing a food labelling policy in
Mexico
Angela Carriedo, Carmen Mena, Claudia Nieto, Jacqueline Alcalde and Simón Barquera
CASE 8 Designing a front-of-package labelling system to encourage healthier
beverage choices in Guatemala
Violeta Chacon, Peter Benson and Joaquin Barnoya
CASE 9 Public-private interaction with the alcohol industry and failures in the
regulation of alcohol in Spain
Ildefonso Hernández-Aguado and Joan R Villalbí
Contents
7
11
18
31
39
46
53
64
80
89
96

6
102
110
121
132
135
138
141
145
CASE 10 From participation to power: how the sugar-sweetened beverage
industry shapes policy through multi-stakeholder coalitions
Craig W Moscetti and Allyn L Taylor
CASE 11 Voluntary agreements and the power of the food industry: the Public
Health Responsibility Deal in England
Clare Panjwani and Martin Caraher
CASE 12 The role of public-private partnerships in childhood obesity prevention
programmes, based on the EPODE experience
Dennis Edell, Jean-Michel Borys and Pauline Harper
COMMENTARY 1 A perspective from the Caribbean
Alaa Samuels, Maisha Hutton and Trevor Hassell
COMMENTARY 2 A perspective from the Americas
Paula Johns and Ana Paula Bortoletto
COMMENTARY 3 A perspective from the Western Pacific region
Katrin Engelhardt
COMMENTARY 4 A perspective from the UK
Cecile Knai and Mark Petticrew
CONCLUSIONS
Je Collin, Rima A and Fabio Gomes

7
Public health and the food and drinks industry: The governance and ethics of interaction FOREWORD
Poor diets are responsible for one in ve deaths globally (Abajobir et al, 2017).
Among high-income countries, the diet-related risk factors of overweight, raised
blood pressure and alcohol are among the top ve leading causes of healthy life
years lost. The leading risk factors of healthy life years lost among low-income
countries are also diet-related and include childhood underweight, micronutrient
deciencies and inadequate breastfeeding. Against this backdrop, overweight and
obesity is rising in all countries and many countries are now challenged by the
double-burden of undernutrition and overweight.
The transformational vision of the 2030 Agenda for Sustainable Development calls
on all countries and stakeholders to work together to end hunger and prevent all
forms of malnutrition by 2030 (United Nations, 2015). The start of the 2030 Agenda
coincided with the launch of the United Nations Decade of Action on Nutrition
(2016-2025) (United Nations and World Health Organization, 2016). This has
boosted the momentum of existing plans for countries to tackle the simultaneous
problems of high rates of child undernutrition, anaemia among women, and rising
rates of overweight, obesity and diet-related non-communicable diseases in all age
groups (World Health Organization, 2015a; 2014).
These global policy frameworks invite international partners, civil society, the private
sector and academia to actively support governments to ensure full implementation
of the global nutrition commitments. There may be dierent forms of engagement
between actors and across sectors, some of them leading to conicts of interest,
whether real or perceived. Thus, while engagement with non-state actors is
important to implement policies and programmes in non-communicable diseases,
adequate rules are needed for eective engagements.
Countries increasingly have to navigate these conicts of interest challenges in
the area of food and nutrition. The World Health Organization (WHO) is committed
to assisting countries with the development of practical tools for addressing and
managing conicts of interest.
In October 2015, WHO held a technical consultation meeting on ‘Addressing and
managing conicts of interest in the planning and delivery of nutrition programmes
at country level’ to inform our approach. Some of the main conclusions of this
consultation included:
• Member states have a duty to ensure that undue inuence – either actual or
perceived – for interests other than the public good is not exerted on individuals or
institutions responsible for public decision-making, in order to not aect integrity
and public trust.
Foreword
FOREWORD
Dr Francesco Branca
Director of Nutrition for Health and Development, World Health Organization

8
Public health and the food and drinks industry: The governance and ethics of interactionFOREWORD
• Conicts of interest can be nancial or non-nancial and a set of tools is needed to
identify and address conicts of interest.
• Policy development should commence with an initial risk assessment which
may involve mapping the dierent interests, understanding corporate tactics and
understanding the level of risk associated with dierent types of engagement with
public and private actors. Member states could establish guidelines on who should
participate in groups responsible for policy in order to avoid conicts of interest
(World Health Organization, 2016).
WHO later reviewed the scientic literature on conicts of interest in policy
development for non-communicable diseases; analysed categories of conicts
of interest, non-state actors and engagement; and reviewed common corporate
tactics across the tobacco and food and beverage industries. WHO also considered
dierent procedures and practices on the prevention and management of conicts
of interest in developing our resources. These included practices adopted by United
Nations agencies, governmental bodies, non-governmental organisations, and
health professional organisations.
WHO has now developed a draft approach on the prevention and management
of conicts of interest in the policy development and implementation of nutrition
programmes at country level (World Health Organization, 2017). This approach is
consistent with WHO’s overall policies and practices, including the WHO Framework
of Engagement with Non-State Actors (World Health Organization, 2015b). There
are plans to test the approach as WHO continues to collect country experiences of
the challenges encountered and the solutions identied in the area of nutrition.
This Casebook publication is timely and welcome. It complements WHO’s work by
providing detailed analyses of dierent types of real-life public-private interactions
to improve nutrition, illustrating how conicts of interest arise, and how these have
been addressed and could be tackled under alternative scenarios to improve
nutrition. The Casebook also highlights the gaps and outstanding challenges
surfacing or arising from this work. It will help to raise awareness of the governance
and ethical issues and challenges underpinning nutrition-related public-private
interactions as an important step towards supporting broader action on avoiding
and managing conicts of interests in nutrition.

9
Public health and the food and drinks industry: The governance and ethics of interaction FOREWORD
References
Abajobir AA et al (2017). Global, regional, and national comparative risk assessment of 84 behavioural, environmental and occupational,
and metabolic risks or clusters of risks, 1990-2016: a systematic analysis for the Global Burden of Disease Study 2016.
The Lancet
, 390
(10100), 1345–1422. http://linkinghub.elsevier.com/retrieve/pii/S0140673617323668 [Accessed 9 October 2017.]
United Nations (2015).
Transforming our World: the 2030 Agenda for Sustainable Development
,
http://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E [Accessed 30 March 2016.]
United Nations, World Health Organization (2016).
United Nations Decade of Action on Nutrition
.
http://www.fao.org/3/a-i6130e.pdf [Accessed 29 June 2017.]
World Health Organization (2014).
WHO Global Action Plan for the Prevention and Control of NCDs 2013-2020
.
http://www.who.int/nmh/publications/ncd-action-plan/en/ [Accessed 3 September 2014.]
World Health Organization (2015a).
Comprehensive Implementation Plan on Maternal, Infant and Young Child Nutrition
. World Health
Organization. http://www.who.int/nutrition/publications/CIP_document/en/ [Accessed 9 October 9 2017.]
World Health Organization (2015b).
Framework of Engagement with Non-State Actors. Report by the Secretariat.
http://apps.who.int/gb/ebwha/pdf_files/EB136/B136_5-en.pdf [Accessed 5 February 2015.]
World Health Organization (2016).
Addressing and Managing Conflicts of Interest in the Planning and Delivery of Nutrition Programmes at
Country Level
.
Technical Report.
Geneva: World Health Organization.
http://www.who.int/nutrition/publications/COI-report/en/ [Accessed 29 June 2017.]
World Health Organization (2017).
Safeguarding Against Possible Conflicts of Interest in Nutrition Programmes
.
http://apps.who.int/gb/ebwha/pdf_files/EB142/B142_23-en.pdf?ua=1 [Accessed 17 December 2017.]
10

11
Public health and the food and drinks industry: The governance and ethics of interaction INTRODUCTION
Background
Global non-communicable disease (NCD) rates are rising rapidly and currently
represent 70% of all deaths worldwide. The burden is particularly severe in
developing countries where three-quarters of NCD-related deaths – 31 million
– occur each year (World Health Organization, 2017). At the heart of this NCD
epidemic are major changes to global diets with shifts away from minimally
processed and healthy foods, towards unhealthy and ultra-processed food and
drinks high in fat, sugar and salt. As a result, nearly 2 billion people around the world
are overweight or obese (The GBD 2015 Obesity Collaborators, 2017), and in low-
income countries more people die from hypertension than from malnutrition (GBD
2015 Risk Factor Collaborators, 2016). The global cost associated with NCDs is
estimated to accumulate to US$ 47 trillion over the next two decades, presenting a
major impediment to economic development (Bloom et al, 2011).
Amidst these alarming disease trends is a tenuous global economy resulting in scal
austerity measures and stretched national budgets. This has led to calls for greater
exibility in collaborating with and receiving nancial support from the commercial
sector. While there may be signicant value in working with the commercial sector,
these interactions may also present a range of governance and ethical challenges,
particularly when the commercial partner is directly responsible for the production
and marketing of unhealthy food and beverages and other products that contribute
to NCDs.
To respond to this policy gap, member states of the World Health Organization
(WHO) have called on its Director General to develop “tools to safeguard against
possible conicts of interest” in the development and implementation of nutrition
policy at the national level (World Health Organization, 2012). This reects rising
concerns around the push for public-private alliances and partnerships to support
the achievement of global health and development commitments such as the UN
Sustainable Development Goals, the UN Decade of Action on Nutrition, and the
WHO global targets on non-communicable diseases (United Nations, 2015; World
Health Organization, 2013; Food and Agriculture Organization of the United Nations
and World Health Organization, 2016).
Issues of governance in public-private interactions are thus central to ensure that
global eorts to tackle non-communicable diseases (NCDs) are undertaken in line
with ethics, transparency, and accountability principles.
Introduction
Authors
Erica Di Ruggiero
Dalla Lana School
of Public Health,
University of Toronto
Greg Hallen
International
Development Research
Centre
Zee Leung
International
Development Research
Centre
Modi Mwatsama
UK Health Forum
INTRODUCTION

12
Public health and the food and drinks industry: The governance and ethics of interactionINTRODUCTION
This Casebook aims to raise awareness and support action on strengthening
governance to avoid and/or mitigate against conicts of interests in dierent country
contexts. The need for this Casebook emerged during a workshop – Improving
governance for better health: Strengthening the governance of diet and nutrition
partnerships for the prevention of chronic diseases – held at the Rockefeller
Foundation Bellagio Conference Centre, Italy, in 2015 (UK Health Forum, 2016a).
It complements an Oxford Bibliography review of the evidence of public-private
partnerships on NCDs (Di Ruggiero et al, 2017). The workshop brought together
20 diverse opinion-forming stakeholders from 14 low-, middle- and high-income
countries across six continents, representing research and academia, civil society
and NGOs, research funding organisations, and the WHO / UN system. The need to
raise such awareness was also echoed in the report of a WHO technical consultation
on addressing and managing conicts of interest in nutrition programmes; WHO
is currently developing tools and guidance to help members address these issues
(World Health Organization, 2016).
Objectives and scope
The specic objectives of the Casebook are:
1 To increase awareness and understanding of the ethical challenges that may
arise from public-private interactions for the prevention of nutrition-related NCDs
across research, policy and practice, with an emphasis on conicts of interest and
governance issues.
2 To advance debate, dialogue and action to strengthen the governance of those
interactions and the avoidance and/or mitigation of conicts of interest.
Selection process
An international Call for Case Studies was launched by the UK Health Forum in
mid-2016 (UK Health Forum, 2016b). This call was published on the UK Health
Forum’s website and disseminated through the networks of the Casebook’s funding
partners and Project Advisory Group. The cases were selected in a two-stage review
process. Abstracts from case studies were screened and assessed for their eligibility
and relevance to the objectives of this Casebook. Authors of eligible and relevant
cases were invited to submit a full-length case study, which was then peer-reviewed
by a group of external reviewers with expertise in NCD prevention, food systems,
ethics, and governance.

13
Public health and the food and drinks industry: The governance and ethics of interaction INTRODUCTION
Full case studies were scored and ranked based on the extent to which they
addressed the following criteria:
1 relevance to the objectives and intended audiences of the Casebook
2 description of background and context for the case, including the drivers of the
interaction
3 clarity and eectiveness of case presentation for the intended audiences, and
4 articulation of the governance issue and its ethical dimensions.
The top scoring case studies were selected for a nal round of peer review
comments and editorial revisions before publication. The case authors completed
forms to declare conicts of interest, and these declarations have been included
within the individual cases.
Oversight of the Casebook project
A Project Advisory Group provided technical support for the production of this
Casebook, including providing input to the scope and design of the Casebook,
identifying external peer reviewers, disseminating the Call for Case Studies and
validating decisions on the eligibility and relevance of accepted cases. This group
was comprised of global health experts from low-, middle- and high-income
countries working for research institutions, funding organisations, civil society
groups, and public sector bodies. In addition an internal management group,
comprised of representatives from the three funders of this Casebook, oversaw the
development of the Casebook.
All individuals involved in the production of the Casebook, including members of the
Project Advisory Group and the internal management group, and peer reviewers,
completed a Declaration of Interest form (including trusteeships, advisory roles, paid
employment or funding). These forms were reviewed by the Project Advisory Group
to ensure that no-one with competing or conicting interests was involved in the
production of the Casebook.
Findings of the Casebook
The cases presented in this Casebook are written by a variety of researchers,
policy practitioners and civil society actors. They cover a range of experiences of
interactions with the commercial sector from across the globe, as briey outlined
below. Each case features an ‘alternative scenario’ which considers whether the
governance and/or ethical issues identied would have been dierent had the
context or circumstances been altered in some way.

14
Public health and the food and drinks industry: The governance and ethics of interactionINTRODUCTION
CASE 1 outlines the potential conict of interests within the Advisory Council of
Mexico’s OMENT (Observatorio Mexicano de Enfermedades No Transmisibles) – an
observatory established to guide policy eorts for obesity prevention and control,
and to become a control unit for surveillance of Mexico’s National Obesity and
Diabetes Prevention and Control Strategy. It also describes the response by the food
and beverage industry to the introduction of taxes on sugar-sweetened beverages
(SSBs) and other regulations to prevent obesity.
CASE 2 examines the Chilean government’s eorts to increase taxes on sugar-
sweetened beverages. It documents the lobbying by the sugar-sweetened beverage
industry against the measures and eorts of civil society actors to support the
process.
CASE 3 describes the ethical and governance challenges encountered by Fiji’s former
Minister of Health in implementing a public-private initiative with the food industry
and the Ministry for Industry and Trade to improve the food supply and public health
outcomes.
CASE 4 describes the eorts of researchers, professionals, activists and policy-
makers in Brazil to draw attention to the issue of conict of interest between public
health and the private food and drinks industry in order to advance the adoption of
regulatory policies to improve food, nutrition and health.
CASE 5 describes the activities and outcomes of two multi-sectoral committees
established by the Canadian government – the Trans Fat Task Group in 2004, and
the Sodium Working Group in 2007 – and explores how these mechanisms may
have stalled regulation by misleadingly suggesting agreement among civil society,
government and industry, and thereby leading to complacency among health
advocates.
CASE 6 examines the wide variety of relationships between the food industry and
a prestigious institute at a university in Chile, ranging from research funding, to
scholarships and joint programmes. The case explores whether these relationships
risk compromising the university’s mandate to conduct independent, high-quality
research and educational activities, as well as its participation in national policy-
making.
CASE 7 describes how a front-of-pack nutrition labelling strategy was developed
in Mexico as part of the national obesity strategy. The case describes how the
outcome involved balancing the interests of the food industry, policy ocials, civil
society members and academic experts.

15
Public health and the food and drinks industry: The governance and ethics of interaction INTRODUCTION
CASE 8 describes a research project in Guatemala to design a front-of-pack nutrition
label to highlight the health risks of sugar-sweetened beverages. It discusses the
merits of commissioning a private marketing rm, which had worked with food and
beverage companies, to design the label.
CASE 9 describes how the alcohol industry in Spain promoted self-regulation and
high-prole partnerships with the government, as a means to curb eorts to increase
alcohol regulations.
CASE 10 outlines some of the risks to public health of partnerships involving food and
beverage companies that produce and market products known to be antithetical to
health. It draws on the experiences and lessons of the Global Health Council’s NCD
Roundtable, which aimed to inuence the global UN and WHO developments on
NCDs.
CASE 11 describes how the calorie reduction initiative of the government’s Public
Health Responsibility Deal in England – which involved the development of reformulation
pledges by multi-national food and drink businesses – resulted in the deection of
public health objectives and the preclusion of adequate monitoring and evaluation.
CASE 12 documents the experience of the EPODE International Network of
childhood obesity prevention programmes. It examines how their multi-stakeholder
and partnerships approach has mobilised resources to support the prevention of
childhood obesity and reductions in the socioeconomic gap in obesity around the
world.
COMMENTARIES – In addition to the 12 cases, four commentaries allow for a broader
discussion of how the ndings of these case studies compared to the experiences
of actors working at the global level as well as in the Caribbean, the Americas, the
Western Pacic and the UK.
CONCLUSIONS – Although these cases and commentaries dier in their geographical
contexts and socio-political histories, common lessons can be identied from their
experiences. These lessons are discussed in greater depth in the Conclusions
section of this Casebook, but in brief:
1 Interactions between the commercial and public sector are numerous and diverse.
2 There is often a lack of transparency and a lack of detailed documentation of these
interactions.
3 There appears to be a general lack of consideration and risk management
undertaken before and during the public-private interactions.

16
Public health and the food and drinks industry: The governance and ethics of interactionINTRODUCTION
Conclusion
We acknowledge that some perspectives are notably absent from this Casebook
– not all geographic regions are represented, and none of the case studies was
submitted by a commercial sector actor. However, we believe that the Casebook
provides an initial but unique contribution to the global health discourse on the
types of interactions that take place between policy-makers, researchers and civil
society actors and the commercial sector in the prevention of diet-related NCDs.
To our knowledge, this Casebook is one of the rst global publications to probe
and unpack the common governance and ethical challenges and opportunities
generated by interactions with the commercial food and drinks sector. Globally, there
appears to be little documentation or transparency on what actually happens within
these interactions. Thus, further research with in-depth analysis and critiques of
these interactions would strengthen our understanding of this eld.
Despite these shortcomings, it is hoped that the Casebook can provide some
guidance to global health actors in recognising, avoiding and mitigating against
governance and ethical challenges which can emerge when interacting with the
commercial sector. It is also hoped that the Casebook will spur greater discussion
and thinking on these complex issues, particularly from the geographic regions
which were under-represented in these cases.
17
Public health and the food and drinks industry: The governance and ethics of interaction INTRODUCTION
Declarations of interest
Erica Di Ruggiero
None declared.
Greg Hallen
None declared.
Zee Leung
None declared.
Modi Mwatsama
Brother is a pricing analysist for Dunnhumby, a subsidiary of the UK retailer Tesco. Brother’s work does not influence my
day-to-day work.
References
Bloom DE, Cafiero ET, Jané-Llopis E, et al (2011).
The Global Economic Burden of Non-communicable Diseases
, Geneva: World
Economic Forum. http://apps.who.int/medicinedocs/documents/s18806en/s18806en.pdf
Di Ruggiero E, Viehbeck S, Mwatsama M, et al (2017). Public-private partnerships in public health research and policy. In: McQueen
D (ed).
Oxford Bibliographies in Public Health
. New York: Oxford University Press (OUP). http://www.oxfordbibliographies.
com/view/document/obo-9780199756797/obo-9780199756797-0161.xml?rskey=jafmWJ&result=1&q=mwatsama#firstMatch
[Accessed 29 June 2017.]
Food and Agriculture Organization of the United Nations and World Health Organization (2016).
United Nations Decade of Action on
Nutrition 2016-2025
. http://www.fao.org/3/a-i6130e.pdf [Accessed 29 June 2017.]
The GBD 2015 Obesity Collaborators (2017). Health effects of overweight and obesity in 195 countries over 25 years.
New England
Journal of Medicine
, 377: 13-27. http://www.nejm.org/doi/10.1056/NEJMoa1614362 [Accessed 29 June 2017.]
GBD 2015 Risk Factor Collaborators (2016). Global, regional, and national comparative risk assessment of 79 behavioural,
environmental and occupational, and metabolic risks or clusters of risks, 1990-2015: a systematic analysis for the Global Burden
of Disease Study 2015.
The Lancet
, 388 (10053): 1659-1724.
http://www.ncbi.nlm.nih.gov/pubmed/27733284 [Accessed 29 June 2017.]
UK Health Forum (2016a).
Improving health through better governance – Strengthening the governance of diet and nutrition
partnerships for the prevention of chronic diseases
. London: UK Health Forum. http://www.ukhealthforum.org.uk/prevention/pie/?
entryid43=55388&q=3082158~UK+Health+Forum+and+the+CIHR-IPPH~
UK Health Forum (2016b). Call for cases: Public-private interactions in nutrition-related non-communicable diseases: Lessons from
research, policy and practice.
http://www.ukhealthforum.org.uk/who-we-are/our-work/ukhf-whats-new/?entryid70=55717 [Accessed 29 June 2017.]
United Nations (2015).
Transforming our world: the 2030 Agenda for Sustainable Development
,
http://www.un.org/ga/search/view_doc.asp?symbol=A/RES/70/1&Lang=E [Accessed 30 March 2016.]
World Health Organization (2012). Sixty-fifth World Health Assembly. Agenda item 13.3. Maternal, infant and young child nutrition.
http://apps.who.int/gb/ebwha/pdf_files/WHA65/A65_R6-en.pdf [Accessed 29 June 2017.]
World Health Organization (2013).
Comprehensive global monitoring framework and targets for the prevention and control of
noncommunicable diseases
. http://apps.who.int/gb/ebwha/pdf_files/WHA66/A66_8-en.pdf?ua=1 [Accessed 3 September 2014.]
World Health Organization (2016).
Addressing and Managing Conflicts of Interest in the Planning and Delivery of Nutrition
Programmes at Country Level. Technical Report
. Geneva: World Health Organization.
http://www.who.int/nutrition/publications/COI-report/en/ [Accessed 29 June 2017.]
World Health Organization (2017).
Noncommunicable diseases: Fact sheet
. World Health Organization.
http://www.who.int/mediacentre/factsheets/fs355/en/ [Accessed 29 June 2017.]
18
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
Authors
Simón Barquera
World Obesity
Federation,
Subcommittee on
Conflict of Interest
Karina Sánchez-
Bazán
World Obesity
Federation,
Subcommittee on
Conflict of Interest
Angela Carriedo
London School of
Hygiene and Tropical
Medicine
Boyd Swinburn
World Obesity
Federation,
Subcommittee on
Conflict of Interest
Corresponding
author
Simón Barquera
Email: sbarquera@
insp.mx
Summary
During 2013, the Mexican government developed a scal reform policy package
which included an initiative to apply a tax to sugar-sweetened beverages (SSBs)
and high-calorie, low-nutrient foods. This initiative was launched in 2014. One
year after its implementation, an evaluation of the eect of the tax found a
reduction of 6-12% in the consumption of SSBs.
Also in 2013, the federal administration launched a National Obesity and
Diabetes Prevention and Control Strategy. As a component of this strategy, it
established the Mexican Observatory on Noncommunicable Diseases (OMENT
– Observatorio Mexicano de Enfermedades No Transmisibles), to guide policy
eorts for obesity prevention and control, and to become a control unit for
surveillance of the national strategy.
OMENT’s Advisory Council included 20 representatives from the public sector,
academia, professional organisations, civil society organisations, industry-
related organisations, and chambers of industry. The two most inuential
organisations participating in OMENT – ConMéxico and the Aspen Institute
Mexico — represent the SSB and high-calorie, low-nutrient food industry, are
sponsored by it, or have strong ties to it. Notably, none of the National Health
Institutes was represented on the Council, nor any of the consumer groups that
had been instrumental in the promotion and approval of the tax on SSBs and
high-calorie, low-nutrient foods, and other initiatives to protect consumers from
unhealthy food.
This case study outlines the potential conicts of interest within the OMENT
Advisory Council. It also describes the response by the food and beverage
industry and associations of SSB producers to the SSB tax initiative and to
other regulations to prevent obesity in the period from 2013 to 2017.
The development of a national obesity and
diabetes prevention and control strategy in
Mexico: actors, actions and conflicts of interest
1
CASE

19
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
Introduction
Since the end of the 1980s, Mexico has experienced an unprecedented rise in
the prevalence of obesity, and diabetes mellitus has become the rst cause of
death (Barquera et al, 2013a; Gómez-Dantés et al, 2016). More than a decade
ago, diverse research groups documented acute changes in the food system,
environment and lifestyles that were associated with this epidemic (Rivera et
al, 2002). Recently the National Ministry of Health declared a national state of
emergency due to this epidemic (Secretaría de Salud, 2016).
In 2009, the Ministry of Health instructed the National Institute of Public Health to
develop the technical basis of a national policy to prevent chronic diseases and
to identify priorities for action. In the following years a number of initiatives were
developed using the best available evidence. Consultations and workshops were
organised with national and international experts, government ocials and food
industry groups. The following initiatives were developed and recommended: a)
an education programme for healthy hydration (Rivera et al, 2008); b) a national
obesity and chronic diseases prevention plan (Barquera Cervera et al, 2010); c) a
front-of-pack labelling system review and recommendations (Barquera et al, 2011);
d) recommendations for taxes on sugar-sweetened beverages and calorie-dense
foods (Barquera et al, 2008); e) guidelines to limit the sale and promotion of calorie-
dense foods and SSBs at elementary schools (Secretaría de Salud and Secretaría
de Educación Pública, 2010; Secretaría de Salud 2010); and f) regulations for
marketing of food and beverages to children (Théodore et al, 2017; Barrera et al,
2016; Théodore et al, 2014; Rincón-Gallardo Patiño et al, 2016).
A strong organised response coordinated by the chambers of industry limited the
progress and implementation of the proposed policies. After a long process and
overcoming many diculties, guidelines to limit SSBs and calorie-dense food at
schools were approved and implemented. The other initiatives were delayed at
negotiation tables until the federal administration’s term (2006-2012) concluded.
Most interactions with SSB and high-calorie, low-nutrient food industry groups were
documented and some of the conicts and push backs have been described in
scientic publications (Charvel et al, 2015; Monterrosa et al, 2015; Barquera et al,
2013b).

20
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
Case
Launch of a novel initiative to reduce consumption of sugar-sweetened beverages
During 2013, in a challenging global economic environment and with large
reductions in the price of oil – which is an important source of revenue for Mexico
– the government developed a scal reform policy package which included an
initiative to apply a tax on SSBs and high-calorie, low-nutrient foods. This initiative,
originally developed by opposition parties, had been supported by civil society
organisations for some years. The convergence of wide support from diverse actors
and the urgent need to increase government revenue were crucial to launching this
policy, which faced very intense opposition lobbying from industry organisations and
chambers of industry. The tax initiative was approved by the Senate and launched
in 2014 with support from opposition parties, civil society organisations, academia,
international organisations such as the World Health Organization, the Pan American
Health Organization and the World Obesity Federation, universities, research centres
and think tanks. One year after its implementation, an evaluation of the eect of the
tax on consumption of SSBs, published in a high-impact peer-reviewed medical
journal, found 6-12% reductions in consumption (Colchero et al, 2016). Some of the
projected health and economic benets of this reduction have also been published
(Sánchez-Romero et al, 2016). In addition, a more recent study showed a sustained
reduction in SSB purchases after two years of implementation of the tax, with an
aggregated average reduction of 7.6% (-5.1 litres per capita per year) (Colchero et al, 2017).
Organised push backs from the SSB and high-calorie food industry to take control of the
National Obesity and Diabetes Prevention and Control Strategy
In 2013, the current federal administration (2012-2018) launched a National Obesity
and Diabetes Prevention and Control Strategy. As a component of this strategy,
the Mexican Observatory on Noncommunicable Diseases (OMENT – Observatorio
Mexicano de Enfermedades No Transmisibles) (OMENT, 2017a) was established.
According to its webpage, the objectives of this observatory are to guide policy
eorts on obesity prevention and control, and to become a control unit for
surveillance of the national obesity and diabetes prevention strategy (OMENT, 2013).
OMENT’s Advisory Council was appointed in September 2014, with the mandate
of supporting the monitoring and impact evaluation of the actions and policies
implemented as part of the National Obesity and Diabetes Prevention and Control
Strategy (Diario Ocial de la Federación, 2014a). The appointees included two
representatives from the public sector, three from academia, four from professional
organisations, six from civil society organisations, two from industry-related
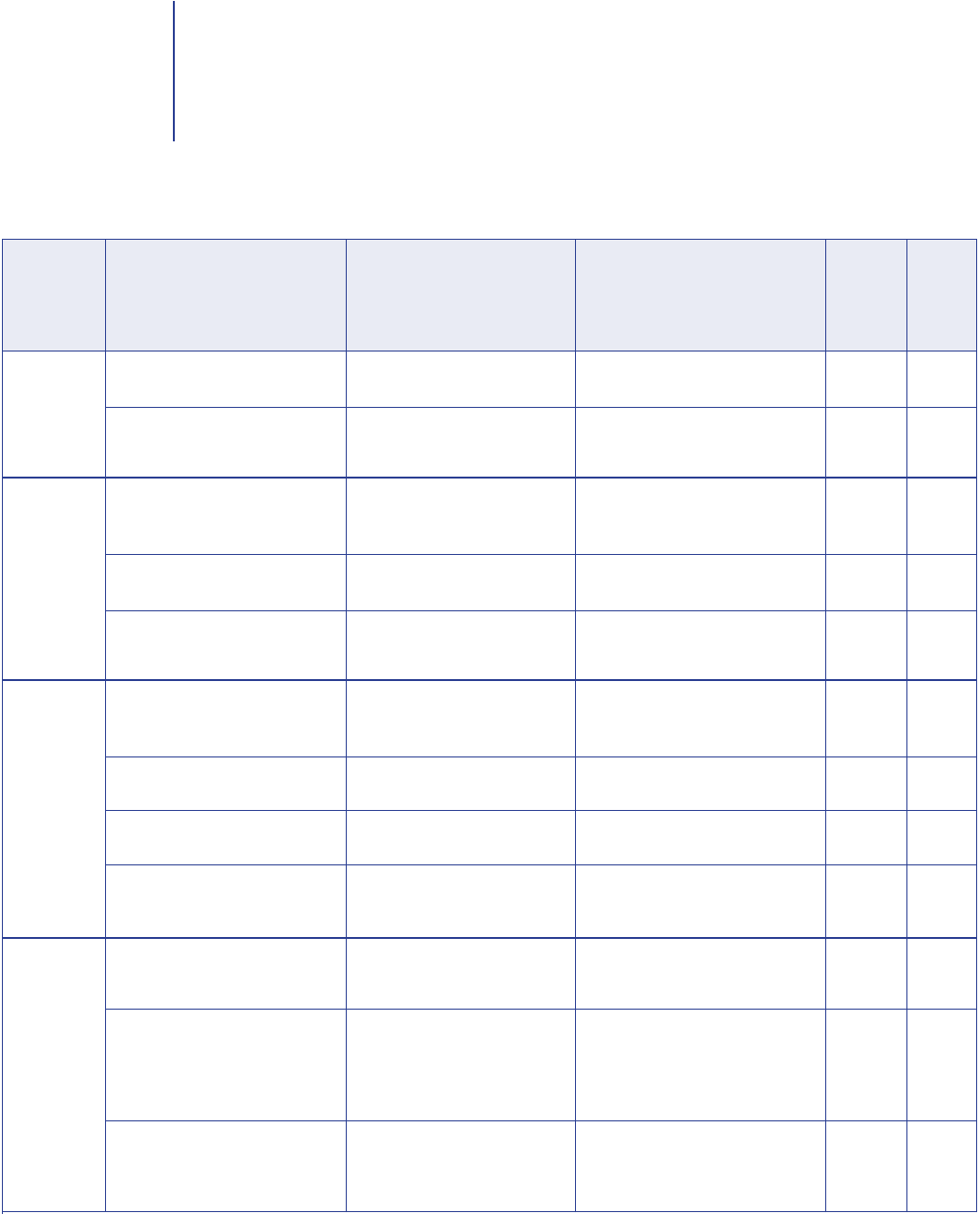
organisations, and three from chambers of industry. Table 1 on page 26 gives details

21
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
of the 20 Advisory Council member organisations and their purpose or main activity,
level of potential conict of interests
1
if any, and level of potential inuence on national
policy. It is relevant to mention that none of the National Health Institutes was
represented on OMENT’s Advisory Council, nor were any of the consumer groups
that had been instrumental in the promotion and approval of the tax on SSBs and
high-calorie, low-nutrient foods, and other initiatives to protect consumers from
unhealthy food.
As Table 1 shows, the two most inuential organisations participating in OMENT –
ConMéxico and the Aspen Institute Mexico — represent the SSB and high-calorie
food industry, are sponsored by it or have strong ties to it. ConMéxico is a council
that groups 43 food and beverage companies such as Bimbo, Ferrero, Danone,
Kellogg’s, Nestlé, Mars, Sigma, Coca-Cola, PepsiCo and Tyson (ConMéxico, 2017). Its
current executive president
2
is an eminent economist who formerly, as a high-level
government ocial, was instrumental in the North America Free Trade Agreement
(NAFTA) negotiation with Canada and the US in 1994. In addition, he was summoned
in early 2017 by the Ministry of Economy to support the current NAFTA re-negotiation
eorts, called by President’s Trump administration (Villamil, 2017). Thus, ConMéxico
is represented by a prestigious personality who is well recognised by most national
and international industrial groups, policy-makers, politicians and government ocials.
NAFTA, which came into force in 1994, established common rules for the
elimination of trade barriers, as well as goods and services barriers, promoted the
mobility of investment ows, and addressed issues such as intellectual property,
and procedures for the resolution of disputes. In relation to taris, the elimination
of barriers was done in dierent ways for dierent products (Centro de Estudios
Internacionales Gilberto Bosques, 2014). Liberalisation of trade in agriculture was
especially dicult to negotiate due to the existing sensibility of the sector. Mexico
was, and still is, at a disadvantage in relation to productivity in comparison with the
US and Canada, which is a problem for Mexican farmers. In the case of sensitive
products like corn and sugar, the transition to the complete liberalisation process
took about 15 years (Food and Agriculture Organization, 2005). The US is by far the
largest exporter of snack foods to Mexico. Additionally, foreign direct investment
from US companies has occurred all along the Mexican food supply chain, from
production and processing to restaurants and retail. US-based soft drink companies,
whose investments in Mexico rose signicantly in the 1990s, dominate this sector
(Clark et al, 2012). Some of these companies are represented by ConMéxico.
1 In the context of this case study, the term ‘conflict of interest’ means any interest declared by an expert that may affect or reasonably be perceived to: (1) affect the
expert’s objectivity and independence in providing advice to the Ministry of Health, and/or (2) create an unfair competitive advantage for the expert or persons
or institutions with whom the expert has financial or business interests (such as adult children or siblings, close professional colleagues, administrative unit or
department). This definition is adopted from the WHO Guidelines for Declaration of Interests.
2 Information valid up to July 2017, according to the organisation’s website http://conmexico.com.mx/sitio/about/estructura/

22
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
The other relevant member of OMENT’s Advisory Council is the Aspen Institute
Mexico, which is relatively unknown by Mexican leaders and interest groups.
However, its current president
3
is the former Dean of the National Mexican
Autonomous University, former president of the Mexican National Academy of
Medicine, and former Minister of Health – easily one of the most recognised leaders
in the health sector. It is relevant to mention that both ConMéxico and the Aspen
Institute have high-level Coca-Cola representatives as members of their Boards.
The potential conicts of interest of the OMENT Advisory Council, presented in Table
1, were assessed using the Typology for a Risk-based Analysis of Conict of Interest
(Global Social Observatory, 2014). The risk-based approach to identifying conicts
of interest is based on the recognition that multi-stakeholder platforms will involve
individual, but especially organisational interests that may be divergent or competing
interests in relation to the objectives and interests of the joint endeavour. In this
typology, conicts are classied as: a) none or minimal conicts that are not likely
to aect policy; b) conicts that might aect policy, but are manageable; c) conicts
that give rise to concern and a need for advice; and d) conicts that are certain
to cause damage to the policy. The level of potential inuence in national policy
proposed was assessed using the Typology of Inuencing Activities (Jones, 2011).
In this typology, the level of inuence is classied as: 1) evidence and advice (low
inuence); 2) public campaigns and advocacy (medium inuence); and 3) lobbying
and negotiation (high inuence).
After the OMENT launch, in 2014 two crucial policies were implemented by the
national regulatory agency (COFEPRIS): 1) modications to the front-of-pack food
labelling system (Diario Ocial de la Federación, 2014b); and 2) regulations for food
and beverage marketing to children (Diario Ocial de la Federación, 2014c). These
were designed without including actors from academia and civil society in the
decision-making expert committees, and were not based on previous scientic work
on the topic (Rivera et al, 2008; Théodore et al, 2014; Barquera et al, 2014; Alianza
por la Salud Alimentaria, 2014).
In general, from 2013 to 2017, the response by the food and beverages industry
and organisations of SSB producers to the SSB tax initiative and other regulations to
prevent obesity, such as front-of-pack labelling, has included the following:
1 Sponsoring and disseminating informal reports minimising or denying the impact
of the tax on SSB consumption and arguing that it has a negative economic eect,
particularly on the poor, creating doubt about the potential documented benets
(Aguilar et al, 2015; Caldiño et al, 2015; Chapa-Cantú et al, 2017).
3 Information valid up to July 2017, according to the organisation’s website http://aspeninstitutemexico.org/

23
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
2 Creating institutes that promote hydration recommendations dierent to the ones
previously published by academia (Coca-Cola México, 2015).
3 Developing alliances with other government sectors for activities such as
supporting the National Council of Science and Technology (Conacyt) awards to
biomedical research (Coca-Cola México, 2016; Lajous and López-Ridaura, 2015).
4 Creating a US$4.7 million media campaign, together with the Ministry of Health, to
promote the current front-of-pack labelling implemented in Mexico — the Guideline
Daily Amounts (GDA) – a system which is proven not to be eective in helping the
population make healthy purchasing decisions (Aguilar, 2017; Rincón-Gallardo et
al, 2016; Tolentino Mayo et al, 2016; OMENT, 2017b).
5 Creating a civil society organisation that promotes healthy lifestyles — Movement
for a Healthy Life (MOVISA) — whose executive president is the same as
ConMéxico’s (MOVISA, 2016).
In addition, the food and beverages industry sponsors and are board members
of civil society organisations that promote physical activity interventions to control
obesity, such as Queremos Mexicanos Activos (Mexicanos Activos, 2016a; 2016b)
and also the Mexican Diabetes Federation (Federación Mexicana de Diabetes,
2017). In these initiatives, messages related to the negative eects of an unhealthy
diet and the consumption of unhealthy products like SSBs are omitted or denied
(Federación Mexicana de Diabetes, 2015; Mexicanos Activos, 2017).
Alternative scenario
Since OMENT is dominated by organisations with potential conicts of interest for
changing food and drink environments, the current scenario for obesity prevention
and control policies in Mexico is challenging. This may or may not change during the
next administration term, which begins in 2018, depending on the political context.
However, in an ideal scenario, public health policy-making should not rely exclusively
on political will, but on scientic evidence-based recommendations and actions.
Diverse conditions could allow for continuity and progress towards improving the
food environment. These include the following:
• Making the prevention and management of conicts of interest a core pillar of
obesity prevention and control policies at all levels. This could be achieved by
having an ocial conicts of interest policy in place. The current perception is that
multi-stakeholder bodies, such as OMENT, are the most inclusive and therefore
eective decision-making platforms. However, when governance criteria and
decision-making processes are not clearly established and made public, there is a
high risk of having biased results and recommendations.

24
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
• Making it mandatory that members of the Advisory Council present an open
declaration of interests. This could strengthen and legitimise the Advisory
Council’s work, and the policy recommendations it supports. The declared
interests should include, among others: a) nancial interests and investments
(stocks, compensation or otherwise); b) nancial support for research activities
provided by the private sector; c) consultancies, employment relationships or other
external professional activities; d) speaking fees from, or sponsored participation
in, lectures, symposia and seminars; and e) memberships in business and/or
philanthropic associations. The declaration of interests is a mechanism that has
been demonstrated to be a powerful tool to prevent conict (Reed, 2008).
•
Having an organisation specialising in transparency to give a third-party opinion
on potential conicts of interest.
A potentially eective mechanism to improve the
Advisory Council’s work could be to have an independent actor — such as an
organisation whose work on transparency and on the prevention and management
of conicts of interest is well recognised — to evaluate or give a third-party opinion
on the potential for conicts of interest for experts and professionals seeking to be
members of the OMENT task force.
•
Comparing progress and results among countries.
This would be desirable. For
example, the INFORMAS Food Environment Policy Index (Swinburn et al, 2013a)
is a valuable tool to identify policy gaps. Comparative rankings across countries
create incentives for governments to develop sound policies, and are convincing
arguments to modify ineective and/or unethical practices.
•
Developing clear decision-making mechanisms with a transparent process
to evaluate policy eorts.
This is fundamental. For example, instead of giving
evaluation and decision-making attributes to an observatory such as OMENT,
whose Advisory Council members have potential conicts of interest, engaging
with the National Council on Evaluation (CONEVAL) – a transparent, well
recognised government agency in charge of evaluating public policy – could result
in more objective evaluations and higher credibility.
25
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
Discussion
Case questions
1 Some of the arguments for including the food and beverages industry on committees
to develop food guidelines, make recommendations, design regulations and evaluate
policies are that: a) they know what can and cannot be done, and how long it would take
to make changes; b) they publicly state that they are also concerned about improving
people’s health; c) they want to be part of the solution; d) a committee must be inclusive
of all society sectors; and e) economy is part of people’s life, and it is important also to
evaluate the economic consequences of proposed interventions. What do you think of
these arguments? Could the SSB and high-calorie food industry be part of the solution? If
so, how and why?
2 Should members from medical societies who are sponsored by food and beverage industries
be accepted into a committee to develop food guidelines? Could this affect the process?
3 How could a mandatory declaration of interests change the composition, operation and
policy recommendations of OMENT’s Advisory Council?
4 Do you consider that multi-stakeholder platforms for public health decision-making are
optimal? Why? How could you ensure transparency, accountability and conflicts of interest
management on those platforms?
Currently, conicts of interest are not discussed in any food and nutrition national
public policy in Mexico, and there are no provisions to avoid the inuence of vested
interests in the decision-making process. It is therefore important to document the
challenges and barriers to implementation that could arise, since a proper framework
to develop obesity prevention policies is lacking. Advances in other countries,
particularly in the Latin American region, and international eorts to document,
monitor and disseminate these policy actions, are essential components to help
implement or rene the National Obesity and Diabetes Prevention and Control
Strategy and associated policies. Initiatives such as the World Obesity Federation
INFORMAS – an international set of protocols to benchmark the food environment,
policy eorts and counter-responses among countries – can accelerate the learning
curve to export successful experiences (such as the Chilean front-of-pack food
labelling systems, the Colombian cycling paths, and the Mexican SSB tax) as soon
as possible to other regions (Swinburn et al, 2013a; Swinburn et al, 2013b).
The food and beverage industry strategies are almost carbon-copies of those used
previously by the Big Tobacco industry: identication of highly prestigious actors
to support their organisations; sponsoring research that tends to support their
interests and be opposed to independent studies; sponsoring medical societies
and social responsibility programmes; high-level lobbying; and creation of institutes
and consensus in agreement with their agenda (Brownell and Warner, 2009;
Freudenberg et al, 2009; Nestle, 2016).
26
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
Fortunately in the academic community and in civil society organisations,
transparency and accountability related to conicts of interest are rapidly becoming
standard practice. Moreover, organisations such as Physicians Without Brands
(Médicos Sin Marca) (Médicos Sin Marca, 2017) are growing throughout Latin
America and in the rest of the world.
Public sector
Academia
Professional
organisations
Civil society
organisations
Minister of Health
(President of the Advisory Council)
Undersecretary of Health Prevention and
Promotion (Technical Secretary of the
Advisory Council)
Mexican Autonomous National University
(UNAM)
(https://www.unam.mx/)
National Polytechnic Institute (IPN)
(http://www.ipn.mx/Paginas/inicio.aspx)
National Association of Universities and
Higher Education Institutions
(http://www.anuies.mx/)
Mexican Academy of Pediatrics
(http://www.academiamexicanadepediatria.
com.mx/)
Mexican Cardiology Society
(http://www.smcardiologia.org.mx/)
Mexican Medicine Academy
(http://www.anmm.org.mx/)
Mexican Public Health Society
(http://www.smsp.org.mx/)
Contrapeso AC
(http://coalicioncontrapeso.org/)
Mexican Diabetes Federation
(http://fmdiabetes.org/)
Queremos Mexicanos Activos AC
(http://www.mexicanosactivos.org/)
-
Ministry of Health branch in charge of
prevention and promotion
Higher education institution
Higher education institution
Association of 187 higher education
institutions
Medical society
Medical society
Medical society
Medical society
Alliance of civil society organisations
that aim to influence public policies
related to obesity prevention
Civil society organisation that promotes
health among patients with diabetes
NGO focused on promoting physical
activity for healthy lifestyles
-
-
-
-
-
Sponsorship of activities by different food
industry companies such as Nestlé.
Funding disclosed on website.
-
-
Sponsorship of some activities by Carlos
Slim Foundation. Funding disclosed on
website.
Funding not disclosed on website.
Has endorsed a book from Coca-Cola and
is sponsored by several food companies.
Funding disclosed on website. (http://
fmdiabetes.org/ibsb-publica-libro-sobre-
importancia-hidratacion/)
Funded by food and beverage companies
such as Bimbo, Coca-Cola FEMSA, Jugos
del Valle, etc. Funding not disclosed on
website.
-
-
MEDIUM
LOW
LOW
LOW
LOW
LOW
LOW
MEDIUM
LOW
LOW
-
-
+
+
+
++
+
+
+
+
++++
+++
Table 1. The Mexican Observatory on Noncommunicable Diseases (OMENT)* Advisory Council and potential
conflicts of interests with health policy recommendations to prevent obesity
Organisation Purpose / main activity** Reasons for potential conflict of
interest
Level of
potential
influence
on national
policy ***
Potential
conflict
of
interest
****
27
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
Industry-
related
organisations
Industry
associations
and chambers
Fundación Este País
Aspen Institute, Mexico
(http://www.aspeninstitutemexico.org/)
Mexican Institute for Competitiveness
(IMCO)
(http://imco.org.mx/home/)
Carlos Slim Foundation
(http://www.salud.carlosslim.org/#1)
Mexican Health Foundation (FUNSALUD)
(http://funsalud.org.mx/portal/)
Mexican Industry Council of Products for
Consumption (ConMéxico)
(https://conmexico.com.mx/sitio/)
National Chamber of the Transformation
Industry (CANACINTRA)
(http://www.canacintra.org.mx/principal/)
Confederación de Cámaras Industriales
de los Estados Unidos Mexicanos
(CONCAMIN)
(http://concamin.mx/)
NGO focused on evidence-based
policy-making
Civil society organisation that promotes
education, leadership and public policy
decision-making
Research centre focused on evidence-
based policy-making
Private, non-profit-making foundation
that focuses on creating solutions to
the main health problems of the most
vulnerable populations in Latin America
Private organisation from industry
focused on channelling philanthropy
and social investment to health
Industry council to promote profitable
development of its associates’ brands
Industry council to promote profitable
development of its associates’ brands
Industry organisation positioned as the
industry political force to promote and
defend their legitimate interests
Partially funded by Queremos Mexicanos
Activos AC. Funding not disclosed on
website. No official website for the
foundation was found.
Holds tight connections with industry. The
President of Coca-Cola Mexico is a member
of the board, and the Executive President
of ConMéxico is one of their economics
advisors. Funding not disclosed on website.
(http://aspeninstitutemexico.org/integrantes/)
Sponsored by the Mexican Council of
Businessmen. The Executive President of
ConMéxico and the CEO of Bimbo were part
of their board. Funding disclosed on website.
(http://imco.org.mx/wp-content/
uploads/2016/01/Informe2014-web.pdf)
Carlos Slim is a former owner of tobacco
companies. Funding disclosed on website.
(http://www.salud.carlosslim.org/nuestros-
aliados/)
Receives funding from Nestlé (Nestlé Fund
for Nutrition) and other food companies.
Funding disclosed on website.
(http://funsalud.org.mx/portal/?page_id=97)
Consortium to oversee interests of their
associates including food industry, alcohol
and tobacco. Funding disclosed on website.
(https://conmexico.com.mx/sitio/about/
nuestros-asociados/)
Consortium to oversee interests of their
associates including food industry, alcohol
and tobacco. Funding disclosed on website.
(http://www.canacintra.org.mx/principal/
index.php/inicio/representatividad/13-
sectores-industriales)
Consortium to oversee interests of their
associates. Funding disclosed on website.
(http://concamin.mx/?page_id=520)
LOW
HIGH
HIGH
HIGH
MEDIUM
HIGH
HIGH
HIGH
++
++++
+++
+
++++
++++
++++
++++
Organisation Purpose / main activity** Reasons for potential conflict of
interest
Level of
potential
influence
on national
policy ***
Potential
conflict
of
interest
****
* OMENT = Observatorio Mexicano de Enfermedades No Transmisibles.
** According to their public information.
*** Level of potential influence on national policy:
LOW = Evidence and advice
MEDIUM = Public campaigns and advocacy
HIGH = Lobbying and negotiation
**** Potential conflict of interest:
+ = None, or minimal conflicts that are not likely to affect policy
++ = Conflicts that might affect policy, but are manageable
+++ = Conflicts that give rise to concern and a need for advice
++++ = Conflicts that are certain to cause damage to the policy
28
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
Acknowledgments
The authors would like to thank Alicia Fernández (University of California, San Francisco) and Cristóbal Cuadrado (Public Health
School, University of Chile) for reading the manuscript and giving valuable recommendations to strengthen the work. This study was
possible in part thanks to an unrestricted grant from Bloomberg Philanthropies to the Mexican National Institute of Public Health.
That grant covered the costs of the panel on conflicts of interest at the International Congress of Public Health Research 2017, which
initiated the reflections and work that form the basis of this case study.
Declarations of interests
Simón Barquera
Processed food and beverage industry:
I was part of the Hydration for Health Initiative expert advisory committee to promote
hydration with water. They covered travel costs to their international experts meeting. I did not receive remuneration. Bonafont
sponsored a research project to my research centre to promote water consumption in the population to reduce metabolic
syndrome. I collaborated in this project.
Pharmaceutical:
Novonordisk, Sanofi-Aventis, Silanes and Ifaceltics sponsored research projects at my centre (descriptive
epidemiological studies from surveys). These studies did not test any drug or specific treatment. The funding was unrestricted
and the funders did not discuss research results or reports.
Weight loss industry:
I have participated in advisory board meetings for Medifast and Herbalife (companies with meal
replacement programmes to treat obesity). In these meetings I presented obesity trends in Mexico and national efforts to prevent and
control the epidemic.
Karina Sánchez-Bazán
Processed food and beverage industry:
Bonafont sponsored a research project at the research centre where I am affiliated. This
project was to promote water consumption in the population to reduce metabolic syndrome. It is relevant to note that I did not
participate in this project.
Pharmaceutical:
Novonordisk, Sanofi-Aventis, Silanes and Ifaceltics sponsored research projects at the research centre where I
am affiliated. The projects were descriptive epidemiological studies from surveys. These studies did not test any drug or specific
treatment. The funding was unrestricted and the funders did not discuss research results or reports. It is relevant to note that I
did not participate in these projects.
Angela Carriedo
None declared.
Boyd Swinburn
None declared.
References
Aguilar A, Gutiérrez E, Seira E (2015).
Taxing calories in Mexico
(preliminary and incomplete draft). Instituto Tecnológico Autónomo
de México. http://cie.itam.mx/sites/default/files/cie/15-04.pdf
Aguilar A (2017). Inicia hoy MOVISA campaña vs obesidad, ‘checa y elige’ 84 mdp, etiquetado foco e IP a largo plazo.
http://www.milenio.com/firmas/alberto_aguilar/movisa-campana-obesidad-televisa-tv_azteca_18_885691442.html
Alianza por la Salud Alimentaria (2014).
El etiquetado frontal nutrimental de bebidas y alimentos en México: a dos años de su
implementación
. http://elpoderdelconsumidor.org/wp-content/uploads/2016/06/Fact-sheet_270616_4-hojas.pdf
Barquera Cervera S, Rivera Dommarco J, Campos Nonato I, et al (2010).
Bases Técnicas del Acuerdo Nacional para la Salud
Alimentaria
. Mexico City: Secretaría de Salud. http://www.promocion.salud.gob.mx/dgps/descargas1/programas/Bases_
tecnicas_acuerdo_nacional_obesidad_29_mar_10_completo.pdf
Barquera S, Hernandez-Barrera L, Tolentino ML, et al (2008). Energy intake from beverages is increasing among Mexican
adolescents and adults.
Journal of Nutrition
, 138 (12): 2454-61. http://jn.nutrition.org/cgi/doi/10.3945/jn.108.092163
Barquera S, Stern D, Tolentino L (2011).
Analysis of the Guideline Daily Amounts (GDA) and its understanding by nutrition students.
Mexico: National Institute of Public Health. https://www.insp.mx/epppo/blog/3225-etiquetado-alimentacion.html
Barquera S, Campos-Nonato I, Aguilar-Salinas C, et al (2013a). Diabetes in Mexico: cost and management of diabetes and its
complications and challenges for health policy.
Globalization and Health
, 9: 3.
http://globalizationandhealth.biomedcentral.com/articles/10.1186/1744-8603-9-3
Barquera S, Campos I, Rivera JA (2013b). Mexico attempts to tackle obesity: the process, results, push backs and future challenges.
Obesity Reviews
, 14 (S2): 69-78.

29
Public health and the food and drinks industry: The governance and ethics of interaction CASE 1: Mexico
Barquera S, Tolentino ML, Safdie M, Lévesque L (2014). National guidelines for healthy nutrition in Mexican schools: an
independent preliminary evaluation.
Obesity Reviews,
15: 258.
Barrera LH, Rothenberg SJ, Barquera S, Cifuentes E (2016). The toxic food environment around elementary schools and childhood
obesity in Mexican cities.
American Journal of Preventive Medicine
, 51 (2): 264-70.
Brownell KD, Warner KE (2009). The perils of ignoring history: Big Tobacco played dirty and millions died. How similar is Big
Food?
Milbank Quarterly
, 87 (1): 259-94. Epub 2009/03/21. doi: 10.1111/j.1468-0009.2009.00555.x
Caldiño E, Minor E, Romero C, Centro de Estudios Económicos de El Colegio de México (2015).
Efectos de la Política de Impuestos
Especiales a Bebidas Saborizadas.
Mexico City: El Colegio de México.
Centro de Estudios Internacionales Gilberto Bosques (2014).
El Tratado de Libre Comercio de América del Norte (TLCAN)
.
A 20
Años de Su Entrada en Vigor
. [Internet]. http://centrogilbertobosques.senado.gob.mx/docs/serieanorte1.pdf
Chapa-Cantú J, Flores-Curiel D, Zúñiga Valero L (2017).
La Industria de las Bebidas no Alcohólicas en México
. Editorial Pearson
and Universidad Autónoma de Nuevo León.
Charvel S, Cobo F, Hernández-Ávila M (2015). A process to establish nutritional guidelines to address obesity: lessons from
Mexico.
Public Health Policy,
36 (4): 426-39.
Clark SE, Hawkes C, Murphy SME, et al (2012). Exporting obesity: US farm and trade policy and the transformation of the Mexican
consumer food environment.
International Journal of Occupational and Environmental Health
, 18 (1): 53-64.
http://dx.doi.org/10.1179/1077352512Z.0000000007
Coca-Cola México (2015). Instituto de Bebidas para la Salud y el Bienestar publica libro sobre la importancia de la hidratación en
las diferentes etapas de la vida.
http://www.mexicanosactivos.org/2016/09/14/mexicanos-activos-otorga-reconocimiento-a-empresas-activas-y-saludables/
Coca-Cola México (2016). Otorgan Conacyt y Coca-Cola premio a investigación biomédica que contribuirá al bienestar general
de la población. http://www.coca-colamexico.com.mx/sala-de-prensa/Comunicados/otorgan-conacyt-y-coca-cola-premio-a-
investigacion-biomedica-que-contribuira-al-bienestar-general-de-la-poblacion
Colchero MA, Popkin BM, Rivera JA, Ng SW (2016). Beverage purchases from stores in Mexico under the excise tax on sugar
sweetened beverages: observational study.
British Medical Journal
, 352: h6704. http://www.bmj.com/lookup/doi/10.1136/bmj.h6704
Colchero MA, Rivera-Dommarco J, Popkin BM, Ng SW (2017). In Mexico, evidence of sustained consumer response two years after
implementing a sugar-sweetened beverage tax.
Health Affairs
, 36 (3): 564-71.
ConMéxico (2017). Nuestros asociados. http://conmexico.com.mx/sitio/about/nuestros-asociados
Diario Oficial de la Federación (2014a). Acuerdo por el que se crea el Consejo Asesor del Observatorio Mexicano de Enfermedades
No Transmisibles. http://www.dof.gob.mx/nota_detalle.php?codigo=5361364&fecha=24/09/2014
Diario Oficial de la Federación (2014b).
Modificación de la Norma Oficial Mexicana NOM-051-SCFI/SSA1-2010, Especificaciones
generales de etiquetado para alimentos y bebidas no alcohólicas preenvasados – Información comercial y sanitaria, publicada el
5 de abril de 2010
. http://www.dof.gob.mx/nota_detalle.php?codigo=5356328&fecha=14/08/2014
Diario Oficial de la Federación (2014c). Lineamientos por los que se dan a conocer los criterios nutrimentales y de publicidad que
deberán observar los anunciantes de alimentos y bebidas no alcohólicas. 15 April 2014.
http://www.dof.gob.mx/nota_detalle.php?codigo=5340694&fecha=15/04/2014
Federación Mexicana de Diabetes (2015). Instituto de Bebidas para la Salud y el Bienestar publica libro sobre la importancia de la
hidratación. http://fmdiabetes.org/ibsb-publica-libro-sobre-importancia-hidratacion/
Federación Mexicana de Diabetes (2017). http://fmdiabetes.org/aliados-de-la-federacion-mexicana-de-diabetes/
Food and Agriculture Organization (2005).
Perspectivas Agrícolas OCDE-FAO, 2005-2014
. Capítulo 3. Azúcar.
http://www.fao.org/docrep/008/y9492s/y9492s07.htm
Freudenberg N, Bradley SP, Serrano M (2009). Public health campaigns to change industry practices that damage health: an
analysis of 12 case studies.
Health Education and Behavior
, 36 (2): 230-49.
Global Social Observatory (2014).
The SUN Movement Toolkit for Preventing and Managing Conflicts of Interest
. Geneva,
Switzerland: Global Social Observatory.
Gómez-Dantés H, Fullman N, Lamadrid-Figueroa H, et al (2016). Dissonant health transition in the states of Mexico, 1990-2013: a
systematic analysis for the Global Burden of Disease Study 2013.
Lancet
, 388 (10058): 2386-2402.
Jones H (2011).
Guide to Monitoring and Evaluating Policy Influence
. London, UK: Overseas Development Institute.
Lajous M, López-Ridaura R (2015). Premio CONACyT-Coca-Cola en medicina: Ciencia y transparencia. NEXOS.
http://www.nexos.com.mx/?p=25994
Médicos Sin Marca (2017). http://www.medicossinmarca.cl/

30
Public health and the food and drinks industry: The governance and ethics of interactionCASE 1: Mexico
Mexicanos Activos (2016a). Mexicanos Activos otorga reconocimiento a Empresas Activas y Saludables.
http://www.mexicanosactivos.org/2016/09/14/mexicanos-activos-otorga-reconocimiento-a-empresas-activas-y-saludables/
Mexicanos Activos (2016b). Sé parte del Reto Empresa Activa y Saludable 2016-2017.
www.mexicanosactivos.org/2016/07/12/se-parte-del-reto-empresa-activa-y-saludable-2016-2017/
Mexicanos Activos (2017).
Manual de Servicios para las Empresas.
http://www.mexicanosactivos.org/wp-content/uploads/2017/01/servicios-empresa.pdf
Monterrosa EC, Campirano F, Mayo LT, et al (2015). Stakeholder perspectives on national policy for regulating the school food
environment in Mexico.
Health Policy Plan
, 30 (1): 28-38.
MOVISA (2016). Empresas y sociedad civil forman Movimiento por una Vida Saludable. MOVISA: September 2016.
http://www.movisa.org.mx/noticia-3.html
Nestle M (2016). Food industry funding of nutrition research: the relevance of history for current debates.
JAMA Internal Medicine,
176 (11): 1685-86.
OMENT (2013). Observatorio Mexicano de Enfermedades No Transmisibles. Universidad Autónoma de Nuevo León.
http://oment.uanl.mx/presentacion-2/
OMENT (2017a). Consejo Asesor. http://oment.uanl.mx/consejo-asesor/
OMENT (2017b). Movisa lanza campaña de educación ‘Checa y Elige’ sobre el etiquetado frontal nutrimental. http://oment.uanl.mx/
movimiento-por-una-vida-saludable-lanza-campana-de-educacion-checa-y-elige-sobre-el-etiquetado-frontal-nutrimental/
Reed Q (2008).
Sitting on the Fence: Conflicts of Interest and How to Regulate Them
. U4 Anti-corruption Resource Centre.
http://www.u4.no/publications/sitting-on-the-fence-conflicts-of-interest-and-how-to-regulate-them
Rincón-Gallardo Patiño S, Tolentino-Mayo L, Flores Monterrubio EA, et al (2016). Nutritional quality of foods and non-alcoholic
beverages advertised on Mexican television according to three nutrient profile models.
BMC Public Health
, 16: 733.
Rincón-Gallardo S, Barquera S, et al (2016).
Análisis de regulaciones y prácticas para el etiquetado de alimentos y bebidas para
niños y adolescentes en algunos países de América Latina (Argentina, Chile, Costa Rica y México) y recomendaciones para
facilitar la información al consumidor.
UNICEF – Instituto Nacional de Salud Pública.
https://www.unicef.org/lac/20161120_UNICEF_LACRO_Etiquetado_Resumen_LR.pdf
Rivera JA, Barquera S, Campirano F, et al (2002). Epidemiological and nutritional transition in Mexico: rapid increase of non-
communicable chronic diseases and obesity.
Public Health Nutrition
, 5 (1a): 113-22.
http://www.journals.cambridge.org/abstract_S1368980002000162
Rivera JA, Muñoz-Hernandez O, Rosas-Peralta M, et al (2008). Consumo de bebidas para una vida saludable: recomendaciones
para la población mexicana.
Salud Pública de Mexico
, 50 (2): 173-95.
http://www.scielosp.org/scielo.php?pid=S0036-36342008000200011&script=sci_arttext
Sánchez-Romero LM, Penko J, Coxson PG, et al (2016). Projected impact of Mexico’s sugar-sweetened beverage tax policy on
diabetes and cardiovascular disease: a modeling study.
PLoS Medicine
, 13 (11): 1-17.
Secretaría de Salud (2010).
Programa de acción en el contexto escolar: Lineamientos técnicos para el expendio o distribución de
alimentos y bebidas en los establecimientos de educación básica
. Mexico: Secretaría de Salud.
Secretaría de Salud (2016). Emite la Secretaría de Salud emergencia epidemiológica por diabetes mellitus y obesidad.
http://www.gob.mx/salud/prensa/emite-la-secretaria-de-salud-emergencia-epidemiologica-por-diabetes-mellitus-y-obesidad
Secretaría de Salud, Secretaría de Educación Pública (2010).
Programa de acción en el contexto escolar. Acuerdo Nacional para la
Salud Alimentaria
. Mexico City: Secretaría de Salud, Secretaría de Educación Pública.
Swinburn B, Sacks G, Vandevijvere S, et al (2013a). INFORMAS (International Network for Food and Obesity/non-communicable
diseases Research, Monitoring and Action Support): overview and key principles.
Obesity Reviews
, 14: 1-12.
Swinburn B, Vandevijvere S, Kraak V, et al (2013b). Monitoring and benchmarking government policies and actions to improve the
healthiness of food environments: a proposed government healthy food environment policy index.
Obesity Reviews
, 14: 24-37.
Théodore F, Juárez-Ramírez C, Cahuana-Hurtado L, et al (2014). Barriers and opportunities for the regulation of food and beverage
advertising to children in Mexico.
Salud Pública de Mexico
, 56 (2): s123-29.
Théodore FL, Tolentino-Mayo L, Hernández-Zenil E, et al (2017). Pitfalls of the self-regulation of advertisements directed at children
on Mexican television.
Pediatric Obesity
, 12 (4): 312-19.
Tolentino Mayo L, Rincón Gallardo Patiño S, Bahena Espina L, et al (2016). Etiquetado nutrimental de alimentos empacados y
bebidas embotelladas. In:
Encuesta Nacional de Salud y Nutrición de Medio Camino: Informe final de resultados.
https://www.gob.mx/cms/uploads/attachment/file/209093/ENSANUT.pdf
Villamil V (2017). Negociadores ‘de peso’ son alineados.
El Financiero.
http://www.elfinanciero.com.mx/economia/negociadores-de-peso-son-alineados.html

31
Public health and the food and drinks industry: The governance and ethics of interaction CASE 2: Chile
Summary
In 2014, the Chilean government proposed the largest major tax reform in
three decades, with the aim of raising revenue for a comprehensive educational
reform. The reform included a proposal to increase taxes on sugar-sweetened
beverages (SSBs).
In response to this, the sugar-sweetened beverage industry in Chile carried
out intensive lobbying, appealing for a defence of autonomy and freedom of
choice for consumers. Some sectors of parliament became prominent allies
of the industry: concerns expressed by those opposing the regulation were
the potential loss of jobs and potential detrimental eects to the economy and
trade.
Civil society started a campaign for a ‘healthy tax reform’, advocating for an
increase of 20 percentage points in SSB taxes, together with a higher level of
taxation for alcohol and tobacco.
The SSB tax reform was introduced, but with an increase of only 5 percentage
points. It also included certain amendments which reduced the impact of
the tax and severely limited the potential eectiveness of the tax to reduce
consumption of SSBs.
Conflicting goals and weakened actions: lessons
learned from the political process of increasing
sugar-sweetened beverage taxation in Chile
Authors
Cristóbal Cuadrado
Escuela de Salud
Pública, Universidad
de Chile
María Teresa
Valenzuela
Escuela de Salud
Pública, Universidad
de Chile
Frente por un Chile
Saludable
Sebastián Peña
Municipalidad de
Santiago, Chile
Frente por un Chile
Saludable
Corresponding
author
Cristóbal Cuadrado
E-mail: ccuadrado@
uchile.cl
2
CASE

32
Public health and the food and drinks industry: The governance and ethics of interactionCASE 2: Chile
Introduction
Chile is facing an increasing burden of non-communicable diseases (NCDs) which
account for at least 53% of all deaths (Departamento de Estadísticas e Información
en Salud (DEIS), 2015). Obesity alone is responsible for 9.1% of deaths (Bedregal
et al, 2008), and 60% of the population is overweight or obese (Ministerio de Salud,
2010). Chile has a high prevalence of unhealthy diets and is one of the three largest
consumers of sugar-sweetened beverages (SSBs) per capita worldwide (Check et
al, 2012; Popkin and Hawkes, 2016; Silver, 2015; Statista, 2015). The link between
consumption of SSBs with obesity and other NCDs (Imamura et al, 2015; Jayalath
et al, 2015; Malik et al, 2013) suggests the need for strong regulatory actions to
increase price, reduce availability and restrict marketing to children (Niebylski et al
2015; Shemilt et al, 2013). Taxation on SSBs represents one of a range of policy
strategies to address this complex problem (Sassi, 2016). The opposition of industry
and its capacity to avoid regulations probably represents one of the most pressing
threats for governments pursuing regulatory policies aimed at improving population
health. This has contributed to a failure to take action (Stuckler and Nestle, 2012).
Case
In 2014, the Chilean government proposed the largest major tax reform for three
decades (Biblioteca del Congreso Nacional de Chile, 2014). The overall goal was
to raise revenue for a comprehensive educational reform, and the reform included a
proposal to increase taxes on SSBs. This increase represented a small proportion
of total revenue, but sparked an intensive political debate involving the public sector,
civil society and private interest groups.
Representatives of the SSB industry raised issues of:
• legality – “arbitrary discrimination”
• equity – “it would aect the poorest families most”
• lack of evidence – “no national studies exist”
• individual choice – “it is all about individual choice”
• side eects – “jobs will be lost”, and
• repression – “the nanny state is coming” (Chilikova, 2016).
It is interesting to note that private industry tried to position themselves on the
moral high ground, appealing for a defence of autonomy and freedom of choice for
consumers.

33
Public health and the food and drinks industry: The governance and ethics of interaction CASE 2: Chile
To do this, the SSB industry carried out intensive lobbying, with a strong media
presence that used increasingly alarming messages to engage the public –
strategies similar to those used by the alcohol and tobacco industries, as has been
discussed in other contexts (Casswell, 2013; Smith et al, 2016; The PLoS Medicine
Editors, 2012). At that time, lobbying activities and corporate nancing for politicians
and political parties were loosely regulated. In this context, the Ministry of Finance
and some sectors of parliament became prominent allies of the industry by opposing
the regulation (Biblioteca del Congreso Nacional de Chile, 2014). At least openly,
the main concerns expressed by those opposing the regulation were the potential
regressivity, loss of jobs and potential detrimental eects to the economy and trade
– very much in line with the industry’s claims. This position created internal conict
within the government, leaving the Ministry of Health in a weakened position. The
reform was managed by the government’s economic teams, and health was treated
as an outsider in the discussion. At the end of the day, the main purpose of the
policy was to increase revenue, not to improve the health of the population.
On the other hand, civil society started a campaign for a ‘healthy tax reform’,
advocating for an increase of 20 percentage points in SSB taxes, together with a
higher level of taxation for alcohol and tobacco. The campaign involved the use
of Twitter storms (which reached 13 million hits between April and July 2014),
newspaper columns, advocacy with the parliament, and public action. Advocates
drew attention to the social responsibility of the state, the importance of protecting
vulnerable populations (i.e. children and low-income groups), and the evident
conicts of interest arising from the participation of the industry in discussions about
legislation.
In this complex political process, the tax reform was passed but was severely
reduced in size, representing an increase of only 5 percentage points, compared
to the evidence-based recommendation for an increase of 20 percentage points
(World Health Organization Regional Oce for Europe, 2015). Two further points
are cause for concern. First, in a last-minute change in parliament, a tax reduction
of 3 percentage points on other ‘low-sugar’ SSBs (less than 15g per 240ml) was
introduced. Secondly, the implementation of the law was made dependent on
industry self-reporting, to the Internal Revenue Oce, the volume of high- and low-
sugar SSBs sold, but with no formal mechanisms for monitoring the data reported
by the industry.
In the context of a highly concentrated market, where a very small number of
companies operate, producing both low- and high-sugar products, the changes
mentioned above gave companies the opportunity to avoid the regulation. Simply
by reporting higher sales of low-sugar products, the industry could compensate

34
Public health and the food and drinks industry: The governance and ethics of interactionCASE 2: Chile
for the potential eect of the increase in tax, without needing to pass on the tax to
the consumer prices. These restrictions severely limited the potential eectiveness
of the tax to reduce consumption of SSBs, and the government lost the window of
opportunity to enforce a relevant and potentially life-saving policy.
It is noteworthy that, in the aftermath of the tax debate, several political scandals
came to the public’s attention, with cases of the industry having undue inuence to
oppose certain legislation, and providing nancial contributions to political parties
and politicians. Also, either knowingly or unknowingly, the National Association
of Beverage Producers had hired a former member of parliament and prominent
political gure to be their external aairs representative within the discussion of
new regulatory attempts, namely, the labelling law for unhealthy products in Chile
(Biblioteca del Congreso Nacional de Chile, 2015).
Alternative scenario
This case study illustrates the need for stronger leadership from the Ministry of
Health, and an institutional design that reinforces broader coordination from dierent
governmental bodies (i.e. the Ministry of Finance, Ministry of Agriculture, Ministry
of Foreign Aairs, and Parliament) to pursue important regulatory actions. Early
incorporation of potential allies such as academia, civil society and consumers’
groups, which proved to be key proponents in favour of industry regulation, can
act as a catalyst for change, counterbalancing the strong opposition from the
industry and disentangling their discourse. Solid technical arguments, political
capacities, and compelling communication strategies are required, but an advanced
understanding of industry’s position and tactics, and of the institutional framework
where the discussion is held, is also needed. The rules of the game matter. They are
key elements that require close attention in any similar political process in the future.

35
Public health and the food and drinks industry: The governance and ethics of interaction CASE 2: Chile
Discussion
Case questions
Engaging civil society in a more effective discussion
1 Could the outcome have been different if the parties opposing the SSB industry had
engaged more effectively in a discussion about ethics, demonstrating how the industry
had co-opted the language of ethics in an attempt to safeguard its own vested interests?
2 Who are the key stakeholders who need to be mobilised to support predictably highly
contested policies?
Providing a strong response to companies’ ‘ethical’ arguments
3 How should the manipulation of the ethics discourse by private companies, with the aim
of protecting their sales, be countered?
Formulation of stronger regulations
4 How can governments respond to industry pressure against regulation?
5 Are there actions that could help to manage the conflicts of interest that arise in complex
political processes?
6 If there had been stronger regulations and democratic processes limiting the influence of
industry, would the outcome of the political process have been different?
Political will
7 Would a stronger leadership from the Ministry of Health and the explicit commitment of
higher political levels of the government be sufficient to counterbalance the influence of
the industry within parliament and in public opinion?
8 How could effective leadership from the Ministry of Health engage other sectors,
particularly the Ministry of Finance, when conflicting interests arise in the policy arena?

36
Public health and the food and drinks industry: The governance and ethics of interactionCASE 2: Chile
The food and beverage industry showed its capacity to have a broad inuence on
policy discussions, engaging actors from academia (Kearns et al, 2016) and public
health organisations (Aaron and Siegel, 2016) as well as politicians (Nestle, 2015).
Public-private interactions in such politically contentious contexts are not innocuous
or even neutral, and most probably undermine public health goals (Brownell, 2012).
As we have seen in this case study, the industry uses the language of ethical
principles such as autonomy and liberty to appeal to the public and policy-makers in
order to protect its self-interest.
This case study highlights the complex scenario where regulatory actions are
discussed with an industry that has the capacity to oppose regulation and uses its
power to inuence decision-makers. This capacity is greater in countries that are
lacking in strict standards to prevent and manage conicts of interest to safeguard
the public interest. Both politicians at the parliament and technical groups at
the Ministries face situations where important conicts of interest could arise.
Transparency and stricter regulation of the conicts of interest between politicians
and the private sector represent a major challenge for countries implementing
regulatory policies. Since 2014, stronger regulations on lobbying and transparency
have started to be imposed in Chile – changes that have been fuelled by political
scandals and the public response (Sahd and Valenzuela, 2016; United Nations,
2017). Making decision-makers politically accountable for their decisions, increasing
public scrutiny (including, for example, full disclosure of any potential conict of
interests), and enforcing higher standards of reporting are desirable steps, although
probably insucient (Loewenstein et al, 2012). Although no rm conclusions can
be drawn on the real inuence that the industry had in the tax discussions, under
the alternative scenario the nal outcome of the policy process would have been
expected to be less favourable to industry and better aligned with public health.
It is unclear if any particular ethical framework was used within the decision-
making process, but it is clear that the process had lacked some basic elements
of fairness, such as transparency and the possibility to appeal against the
decision. Developments from the ethics literature, such as the ‘accountability for
reasonableness’ framework (Daniels, 2000; Martin et al, 2002), could provide a
sound basis for developing stronger institutional frameworks that aim to ensure
fair and legitimate decision-making processes, and that regulate the eects of
competing interests in the public policy arena.
37
Public health and the food and drinks industry: The governance and ethics of interaction CASE 2: Chile
Acknowledgments
The authors would like to thank Professor Renaud Boulanger for his important contributions and suggestions for the ethical
discussion of the case, and two anonymous reviewers for their commentaries, allowing further reflections and improvement of the
overall case study structure.
Declarations of interests
Cristóbal Cuadrado
Ministerio de Salud (Ministry of Health) Chile, Pan-American Health Organization, World Food Program, World Bank, Colegio
Médico de Chile (Chilean Medical Association), NGO Médicos Sin Marca:
• Contracts as consultant for different research-related activities for both national and international governmental institutions.
Honoraria fees dependent on the contract.
• Technical Secretariat at the Department of Public Policy of the Chilean Medical Association. Paid employment.
• Director of the NGO Médicos Sin Marca (Physicians without Brands), promoting a critical culture on the relationships
between industry and physicians in Chile.
Ad honorem
position (no salaries, fees or other financial incentives are received).
María Teresa Valenzuela
None declared.
Sebastián Peña
Vital Strategies (as part of a project with Bloomberg Philanthropies), National Institute for Health and Welfare, and Finnish
Foundation for Alcohol Studies:
• Contract as a consultant with Vital Strategies in support for the Mayors Challenge 2016 from Bloomberg Philanthropies (2017).
• Consultant for the National Institute for Health and Welfare for the FRESHER Project (funded by the European Union) (2017).
• Grant for PhD studies from the Finnish Foundation for Alcohol Studies (2017).
References
Aaron DG, Siegel MB (2016). Sponsorship of national health organizations by two major soda companies.
American Journal of
Preventive Medicine
, 52: 20-30. http://doi.org/10.1016/j.amepre.2016.08.010
Bedregal P, Margozzini P, Gonzalez C (2008).
Informe Final: Estudio de Carga de Enfermedad y Carga Atribuible, Chile 2007.
Santiago de Chile: Ministerio de Salud.
Biblioteca del Congreso Nacional de Chile (2014).
Historia de la Ley No 20.780. Reforma Tributaria que Modifica el Sistema de
Tributación de la Renta e Introduce Diversos Ajustes en el Sistema Tributario.
Biblioteca del Congreso Nacional de Chile.
Biblioteca del Congreso Nacional de Chile (2015).
Ley 20.606 sobre Composición Nutricional de los Alimentos y su Publicidad.
Biblioteca del Congreso Nacional de Chile.
Brownell KD (2012). Thinking forward: the quicksand of appeasing the food industry.
PLoS Medicine
, 9 (7): 1-2.
http://doi.org/10.1371/journal.pmed.1001254
Casswell S (2013). Vested interests in addiction research and policy. Why do we not see the corporate interests of the alcohol
industry as clearly as we see those of the tobacco industry?
Addiction
, 108(4): 680-85. http://doi.org/10.1111/add.12011
Check D, Dodson M, Kirk C (2012). Americans drink more soda than anyone else: a map of soda consumption in 80 countries.
http://www.slate.com/articles/health_and_science/map_of_the_week/2012/07/map_of_soda_consumption_americans_drink_
more_than_anyone_else_.html [Accessed 1 February 2016.]
Chilikova K (2016).
An Assessment of the Political Factors Associated with a Tax Increase on Sugar Sweetened Beverages in Chile.
Georgetown University.
Daniels N (2000). Accountability for reasonableness.
British Medical Journal,
321:1300-01. http://doi.org/10.1136/bmj.a1850
Departamento de Estadísticas e Información en Salud (DEIS) (2015). Defunciones y Mortalidad por Causas – 2000 a 2011. http://
www.deis.cl/?p=2541 [Accessed 11 December 2015.]
Imamura F, O’Connor L, Ye Z, et al (2015). Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit
juice and incidence of type 2 diabetes: systematic review, meta-analysis, and estimation of population attributable fraction.
British
Medical Journal
, 351: h3576. http://doi.org/10.1136/bmj.h3576

38
Public health and the food and drinks industry: The governance and ethics of interactionCASE 2: Chile
Jayalath VH, de Souza RJ, Ha V, et al (2015). Sugar-sweetened beverage consumption and incident hypertension: a systematic
review and meta-analysis of prospective cohorts.
American Journal of Clinical Nutrition
, 102: 914-21.
doi: 10.3945/ajcn.115.107243.
Kearns CE, Schmidt LA, Glantz SA (2016). Sugar industry and coronary heart disease research: a historical analysis of internal
industry documents.
JAMA Internal Medicine
, 176 (11): 1680-85. doi:10.1001/jamainternmed.2016.5394
Loewenstein G, Sah S, Cain DM (2012). The unintended consequences of conflict of interest disclosure.
Journal of the American
Medical Association,
307 (7): 669-70. http://doi.org/10.1001/jama.2012.154
Malik VS, Pan A, Willett WC, Hu FB (2013). Sugar-sweetened beverages and weight gain in children and adults: a systematic review
and meta-analysis.
The American Journal of Clinical Nutrition
, 98 (4): 1084-102. doi: 10.3945/ajcn.113.058362
Martin DK, Giacomini M, Singer PA (2002). Fairness, accountability for reasonableness, and the views of priority setting decision-
makers.
Health Policy
, 61 (3): 279-90.
Ministerio de Salud (2010).
Encuesta Nacional de Salud. Chile 2009-2010
. Ministerio de Salud.
Nestle M (2015).
Soda Politics: Taking on Big Soda (and Winning)
. New York: Oxford University Press.
Niebylski ML, Redburn KA, Duhaney T, Campbell NR (2015). Healthy food subsidies and unhealthy food taxation: a systematic
review of the evidence.
Nutrition,
31 (6): 787-95. http://doi.org/10.1016/j.nut.2014.12.010
The PLoS Medicine Editors (2012). PLoS Medicine series on Big Food: the food industry is ripe for scrutiny.
PLoS Medicine
, 9 (6):
e1001246. http://doi.org/10.1371/journal.pmed.1001246
Popkin BM, Hawkes C (2016). Sweetening of the global diet, particularly beverages: patterns, trends, and policy responses.
The
Lancet Diabetes and Endocrinology
, 4 (2): 174-86. http://doi.org/10.1016/S2213-8587(15)00419-2
Sahd J, Valenzuela C (2016).
Lobby Law in Chile Democratizing Access to Public Authorities
. Open Government Partnership. http://
www.opengovpartnership.org/sites/default/files/report_Lobby-law-in-Chile.pdf
Sassi F (2016). Taxing sugar.
British Medical Journal,
352: h6904. http://doi.org/10.1136/bmj.h6904
Shemilt I, Hollands GJ, Marteau TM, et al (2013). Economic instruments for population diet and physical activity behaviour change:
a systematic scoping review.
Plos One,
8 (9): e75070. http://doi.org/10.1371/journal.pone.0075070
Silver M (2015). Guess which country has the biggest increase in soda drinking. http://www.npr.org/sections/
goatsandsoda/2015/06/19/415223346/guess-which-country-has-the-biggest-increase-in-soda-drinking [Accessed 1 February
2016.]
Smith K, Dorfman L, Freudenberg N, et al (2016). Tobacco, alcohol, and processed food industries – Why do public health
practitioners view them so differently?
Frontiers in Public Health
, 4: 64. http://doi.org/10.3389/fpubh.2016.00064
Statista (2015). Annual per capita consumption of Coca-Cola Company’s beverage products from 1991 to 2012, by country (in
servings of 8-fluid ounce beverages). http://www.statista.com/statistics/271156/per-capita-consumption-of-soft-drinks-of-the-
coca-cola-company-by-country/ [Accessed 1 February 2016.]
Stuckler D, Nestle M (2012). Big food, food systems, and global health.
PLoS Medicine
, 9 (6): 7.
http://doi.org/10.1371/journal.pmed.1001242
United Nations (2017). Chile: Anti-corruption and transparency in public administration – United Nations and the Rule of Law.
https://www.un.org/ruleoflaw/blog/portfolio-items/chile-anti-corruption-and-transparency-in-public-administration/ [Accessed 5
April 2017.]
World Health Organization Regional Office for Europe (2015).
Using Price Policies to Promote Healthier Diets
. Copenhagen: World
Health Organization Regional Office for Europe. http://doi.org/10.13140/RG.2.1.4853.3923
39
Public health and the food and drinks industry: The governance and ethics of interaction CASE 3: Fiji
Summary
Non-communicable diseases (NCDs) account for 80% of all deaths in Fiji, an
archipelago of just over 330 islands in the Pacic region. Globally, increasing
consumption of processed food products, including sugar-sweetened
beverages (SSBs), has been an important contributor to the high rates of
obesity and NCDs. In 2009, the Minister of Health in Fiji initiated a public-private
initiative (PPI) with the food industry and the Ministry for Industry and Trade, with
the aim of improving the food supply, and, ultimately, public health outcomes.
This case study provides a reective and narrative description of the former
Minister’s experience, from 2009 to 2014, while engaged in the development
and implementation of this PPI. The ethical issues of conicts of interest of
the food industry were never discussed, and the SSB subgroup, made up
of ve major industry actors in that sector, was allowed to work on matters
of marketing policy, reformulation and practice re-modelling alongside
public health advocates and health ocials. The industry engaged early by
participating in regular meetings. Consultations with food industry members
were held to discuss and agree targets, standards, marketing and product
availability. However, major ethical dilemmas emerged when trade and national
development were given precedence over public health concerns. For example,
the industry tried to shift the blame away from SSBs, by focusing on physical
activity promotion. It also used self-regulation to rebut eorts by the Ministry of
Health to move forward with legal, regulatory controls on marketing of unhealthy
products to children. In addition, members of the industry lobbied senior ocials
in other government departments, while avoiding further engagement with the
Ministry of Health. Governance was another issue, and regular non-attendance,
changes of representatives and a lack of involvement from the Ministry for
Industry and Trade became logistical obstacles to eective policy development.
In Fiji, since 2013, there have been no reductions in SSB marketing or
availability, no new products with lower sugar content made available, and no
evidence of any plans by the industry for this to happen. The self-regulation
approach has not been as successful as it was expected to be.
In this case study, we discuss a PPI with the SSB industry and its associated
ethical challenges.
Sugar-sweetened beverages, non-communicable
diseases and the limits of self-regulation in Fiji
Authors
Neil Sharma
Fiji College of
General Practitioners
Former Minister of
Health, Fiji, 2009-14
Melissa Mialon
Department of Health
Sciences, University
of York, UK
Corresponding
author
Melissa Mialon,
Email:
mialon@york.ac.uk
or
melissa_mialon@
hotmail.fr
3
CASE

40
Public health and the food and drinks industry: The governance and ethics of interactionCASE 3: Fiji
Introduction
Non-communicable diseases (NCDs) account for 80% of all deaths in Fiji, in part
driven by the consumption of unhealthy diets, which have contributed to high rates
of obesity, with 30% of the population being obese (World Health Organization,
2014). Globally, increasing consumption of processed food products, including
sugar-sweetened beverages (SSBs), has been an important contributor to the
escalating NCD crisis (Nestle, 2015).
In 2007, during the 7th Pacic Health Ministers meeting in Vanuatu, it was agreed
that national food summits would be organised annually across the dierent
countries of the Western Pacic region and would include, as standard practice,
all stakeholders (World Health Organization Western Pacic Region, 2010). In Fiji,
these consultations started in 2009 and were attended by representatives of the
government in agriculture, health, industry and trade, and education, along with
key food importers, wholesalers, manufacturers and exporters of fresh and locally
processed foods (The Fijian Government, 2009). Development partners with a
regional oce based in Fiji were also invited to the consultations. These included
the Pacic Community, the World Health Organization (WHO), the United Nations
Children’s Fund (UNICEF) and the Food and Agriculture Organization of the United
Nations (FAO). The Consumers Council of Fiji, a not-for-prot, also participated in
these consultations. Fiji’s National Food and Nutrition Centre (NFNC), the NCD team
at the Ministry of Health, the Pacic Research Center for the Prevention of Obesity
and Non-Communicable Diseases (C-POND) from Fiji National University, and the
Australian Agency for International Development (AusAID) oversaw the organisation,
communication and follow-up of these events.
Neil Sharma, one of our authors and then Minister of Health in Fiji, initiated a
public-private initiative (PPI) with the food industry, with the aim of improving food
supply and public health outcomes through several measures, including salt and
sugar reduction in food products, healthier cooking oil options, and educational
programmes in schools (Ministry of Health, Fiji, 2009). One of the specic objectives
was to inform and collaborate with the food industry to curtail public consumption
of SSBs and facilitate greater availability of healthier alternatives, alongside supply
changes for other categories of food products.
The decision, by the Ministry of Health, to include all stakeholders in the PPI was
made in an open and transparent manner, anticipating a good working relationship,
as is usually the case in the Pacic cultures, where public health would be at the
centre stage in all discussions. The PPI was to be a test case for the regional small
islands territories to emulate at their own paces. In addition to the stakeholders’
consultations with the Ministry of Health, the National Food and Nutrition Centre

41
Public health and the food and drinks industry: The governance and ethics of interaction
CASE 3: Fiji
conducted regular meetings with individual industry actors with the same objectives.
In this case study, we discuss a PPI that involved the SSB industry in Fiji, and its
associated ethical challenges. We provide a reective and narrative description
of the former Minister’s experience, from 2009-2014, while engaged in the
development and implementation of this PPI.
Case
The industry engaged early, and actively participated in the national and individual
consultations. Because the industry was supportive and open to discussion, the
planning and implementation of this PPI, led by the Ministry of Health, did not involve
any assessment of potential ethical or related issues. However, by 2010-2011,
some subtle ethical challenges started to emerge, including a lack of transparency
from the food industry, and failure to progress and/or to report on progress by the
food industry. Regular non-attendance, changes of representatives and a lack of
involvement from the Ministry for Industry and Trade also became logistical obstacles
to eective policy development.
These challenges became apparent when, in 2013, some food industry actors
formed the Fiji Beverage Group, in response to calls during the consultations for
industry to collaborate in sector-specic groups to improve health. This group was
made up of ve major actors: Coca-Cola Amatil Fiji/Coca-Cola Oceania (Beverage
Group Representative); Frezco Beverages Ltd; Motibhai Group of Companies;
Pinto Industries Ltd; and The Tappoo Group of Companies. They developed a
Memorandum of Understanding (MOU) in August 2013, which they had initially
intended to be signed with the Ministry of Health, but was nally approved by the
members of the group only (The Fiji Beverage Group, 2013). This MOU made a
number of commitments for new products, package size reductions, and limits on
marketing to children, and voluntarily committed to report to the Ministry of Health
annually on its progress. Public health advocates suggested that the group used
this MOU to rebut eorts by the Ministry of Health to move forward with controls
on the marketing of unhealthy food products to children, in line with the WHO
recommendations (Mialon et al, 2016; World Health Organization, 2010). The most
signicant weakness of this MOU, in comparison with the proposed legislation on
marketing, apart from its self-regulatory nature, was that it included only a small
number of food industry actors. This would then leave the majority of industry actors
to continue with their current marketing practices, including those targeting children.
In 2015, public health advocates noted that, since the launch of this MOU, no
evidence of its implementation was provided, despite requests from the Ministry of
Health (Mialon et al, 2016). It therefore appears that most commitments made early
on by the SSB industry were not followed.

42
Public health and the food and drinks industry: The governance and ethics of interactionCASE 3: Fiji
In parallel, the SSB industry immediately started to employ corporate political
strategies, when they began to shift the blame for NCD and obesity away from SSBs
and onto physical inactivity and energy balance (Mialon et al, 2016). For example,
Coca-Cola organised the Fiji Secondary Schools Athletics Competition, a major
annual event held in the capital city (Makaba, 2015). The campaign on physical
activity from the SSB industry was supported by overseas industry consultants and
experts, particularly from transnationals (Neil Sharma, personal communications and
meetings; records of these meetings are not available in the public domain). These
tactics were further complicated by an emphasis on personal responsibility. All these
messages were widely advertised (Mialon et al, 2016).
The SSB group was made aware that, if compliance to the PPI was not forthcoming,
SSB taxes could be recommended by the Ministry of Health (Neil Sharma, personal
communications). The industry started lobbying high-ranking ocials to avoid these
taxes, focusing on its work to promote physical activity (and how this would balance
energy intake from SSBs) and on its employment of local people (Neil Sharma,
personal communications). The Coca-Cola group threatened to relocate their
operations to another island territory, Western Samoa, whilst the suppliers of Pepsi-
Cola threatened not to proceed with developing their new plant in Fiji, withdrawing
employment opportunities for Fijians (Neil Sharma, personal communications).
Around 2013, no progress was made with the PPI, and the Ministry of Health started
developing tax proposals and a call for marketing restrictions. The Ministry was
transparent throughout in its dealings with the industry, sharing the draft proposals
at the consultations (Neil Sharma, personal communications and meetings).
Nevertheless, heavy lobbying by the industry to the Ministry for Industry and Trade,
without the involvement of the Ministry of Health or any other sector, resulted in an
inconsistent response from the government to the industry calls and demands (Neil
Sharma, personal communications; records of these meetings are generally not
circulated). The lack of transparency from the industry in the planning and outcomes
of these meetings, and additional meetings between individual companies, further
added to the problem.
The general elections took place in 2014, resulting in a change of health leadership
and some reduction in the budgetary funding for NCDs.
It is important to note that, in parallel to the PPI, several not-for-prot organisations
worked collectively, and oered an unprecedented level of support for these taxes
and marketing restrictions. The Alliance for Healthy Living – led by Diabetes Fiji
and the Consumer Council of Fiji, along with faith-based organisations, women’s
groups and other social clubs with health advocacy interests – was formed and

43
Public health and the food and drinks industry: The governance and ethics of interaction CASE 3: Fiji
formally endorsed by the Ministry of Health in 2014. However, following some initial
consultation forums and a high media prole, the activities of the group waned,
mainly due to a lack of time, leadership (which could have shaped a strategic
direction), as well as funding challenges.
In conclusion, in Fiji, since 2009 and the launch of the PPI mentioned in this case
study, there have been no reductions in SSB marketing or availability, no new
lower-sugar products made available, and no evidence of any plans by the industry
to make this happen. The PPI and self-regulation approach have not been as
successful as they were expected to be. This highlights the ethical issues of conict
of interest in this PPI, driven by the prot orientation of the SSB industry.
Alternative scenario
From this case study, it became clear that a concerted approach by the government
wherein dierent ministries worked in close consultation was needed, with strong
buy-in and understanding from all sectors.
In areas where public health was at stake, ethical issues should have been
addressed, and an ethics committee should have been consulted, well before and
during the consultations with the industry. In addition, ocials were probably not
technically prepared to handle the interaction with the industry.
At that period, Fiji was in political transition, with an interim government in place,
and public participation in politics was quite limited. In a dierent political context,
wide public consultation may have helped. In addition, funding challenges faced by
not-for-prot organisations could have been tackled with a stronger leadership and
involvement of development partners (including funding agencies), and could have
ensured that all stakeholders were represented in the policy-making process.
There could have been a formal evaluation and monitoring of the PPI to ensure that
the industry was meeting the planned objectives.
Mialon et al (2016) have proposed a list of policies and measures that, if developed
and shared in the public domain, could help increase the transparency and
accountability of the government and the food industry in Fiji. For the specic case
study described here, these could have included:
• a list and content of the submissions to public consultations from the food industry
on issues related to diet and public health
• a list of meetings between food industry representatives and Ministers, ocials
and/or representatives of the government, and minutes of those meetings (and
other reports), and
44
Public health and the food and drinks industry: The governance and ethics of interactionCASE 3: Fiji
• all correspondence (including emails) between food industry representatives and
ocials and/or representatives from the government.
With more strategic planning initially, the Ministry of Health and its partners might
have foreseen the likely considerable opposition to its approaches, and mounted
a more strategic and proactive approach to rebutting the countermoves of the
industry.
Discussion
Case questions
1 Should the terms and conditions of engagement between the government and the industry
in this public-private initiative have been discussed with an ethics committee prior to that
engagement?
2 Could consultation with the SSB group have been tackled differently with greater public
health impact?
3 What is the role of self-regulation by the SSB industry in an urgent public health issue?
Fiji was ahead of many other countries in actively pursuing a PPI with the food
industry and addressing the NCD crisis. Wide consultations with the food industry
were initiated with considerable time and resource investments by the Ministry of
Health, and involved a diverse range of stakeholders. Despite initial buy-in from
industry and a seemingly transparent and positive relationship, the concerted
response by industry to undermine the approach of the Ministry of Health was
overwhelming.
Similarly to the tactics employed by the tobacco industry decades ago, the SSB
industry is rejecting the evidence that links its products with obesity and NCDs.
More work is needed globally to develop tools, which can be applied nationally,
to engage with the industry, helping especially low- and middle-income countries
to take matters forward. Taxation and other regulatory approaches are a globally
recommended strategy to support the prevention and control of NCDs. The food
industry could play an active role, mostly during the implementation phase of the
policy process.
The development impact of NCDs in middle-income countries such as Fiji is a
mammoth challenge given the limited scal and healthcare resources available.
When the international food industry takes on a totally ‘for-prot’ approach with
corporate political strategies directed mostly to economic gains, public health seems
to be the victim. National development cannot take place without public health
concerns being factored in to any short- to medium-term national strategic plan.
45
Public health and the food and drinks industry: The governance and ethics of interaction CASE 3: Fiji
Acknowledgments
The authors would like to thank Dr Devina Nand and Dr Wendy Snowdon who provided some insight and information on the issues
in this manuscript, although they may not agree with all of the interpretations and conclusions of this paper. The authors would also
like to thank the anonymous reviewers, for their helpful comments and suggestions, and Dr Modi Mwatsama, from the UK Health
Forum, for her continuous support.
Declarations of interests
Neil Sharma
None declared.
Melissa Mialon
None declared.
References
The Fiji Beverage Group (2013).
Memorandum of Understanding: Supporting Healthy Active Lives for People in Fiji.
Fiji Islands.
The Fijian Government (2009).
Fiji Food Summit began on a high note
. Fiji Islands. http://www.fiji.gov.fj/Media-Center/Press-
Releases/Fiji-food-summit-begins-on-a-high-note.aspx [Accessed May 2017.]
Makaba J (2015). Enjoy the games says Watkins.
Fiji Times
, 24 April 2015.
Mialon M, Swinburn B, Wate J, et al (2016). Analysis of the corporate political activity of major food industry actors in Fiji.
Globalization and Health
, 12: 18. doi 10.1186/s12992-016-0158-8
Ministry of Health, Fiji (2009).
Fiji Food Summit 2009
. Fiji Islands.
Nestle M (2015).
Soda Politics: Taking on Big Soda (and Winning)
.Oxford: Oxford University Press.
World Health Organization (2010).
Set of Recommendations on the Marketing of Foods and Non-alcoholic Beverages to Children
.
Geneva: World Health Organization.
World Health Organization (2014).
Global Status Report on Noncommunicable Diseases 2014
. Geneva: World Health Organization.
World Health Organization Western Pacific Region (2010).
Pacific Food Summit
. Port Vila, Vanuatu: World Health Organization.
46
Public health and the food and drinks industry: The governance and ethics of interactionCASE 4: Brazil
Authors
Inês Rugani Ribeiro
de Castro
State University of
Rio de Janeiro, Brazil
Camila Paes de
Carvalho
State University of
Rio de Janeiro, Brazil
Paulo Castro Jr
National School of
Public Health Sérgio
Arouca, Fiocruz,
Brazil
Luciene Burlandy
Fluminense Federal
University, Brazil
Veruska Alexandre
Federal University of
Goiás, Brazil
Ana Feldenheimer da
Silva
State University of
Rio de Janeiro, Brazil
Luciana Maldonado
State University of
Rio de Janeiro, Brazil
Daniela Canella
State University of
Rio de Janeiro, Brazil
Corresponding
author
Inês Rugani Ribeiro
de Castro
Email: inesrrc@uol.
com.br
Summary
In Brazil, the issue of conict of interest between public health and the private
food and drinks industry has historically received little attention, and the private
sector’s resistance to regulatory measures has prevented progress on public
policies in food and nutrition.
In 2012, a collective of researchers, professionals, activists and policy-makers
– the Frente pela Regulação da Relação Público Privado em Alimentação e
Nutrição (FRRPPAN – Front for the Regulation of the Public-Private Relationship
in Food and Nutrition) was established, to take political action to advance
regulatory strategies. This collective increased awareness of the conict of
interest issue in Brazil.
In 2014, a Task Force to Promote Bills of Law to Regulate Food Advertising,
Labelling, and Environments was created, bringing together members of civil
society, government and academia with the aim of developing concerted
political action to advance the regulatory agenda.
In 2016, a third collective – the Alliance for Adequate and Healthy Eating – was
formed, consisting of public interest civil society organisations, professionals,
associations and social movements. Its purpose is collective advocacy aimed
at greater political inuence in the area of food and nutrition, independent from
government and free from conicts of interest with the food industry.
This case study describes how linkage between these three initiatives has
allowed more incisive action in the promotion and defence of regulatory
restrictions on the promotion of unhealthy food products and practices in Brazil.
It also looks at the eorts made to develop mechanisms to safeguard against
and mitigate conicts of interest in academic institutions.
Political action by researchers, professionals,
activists and policy-makers to advance the food
and nutrition regulatory agenda in Brazil
4
CASE

47
Public health and the food and drinks industry: The governance and ethics of interaction CASE 4: Brazil
Introduction
The core activities of corporations involved in food production, agricultural inputs
(e.g. seeds, pesticides, fertilisers and machinery), and retail food sales have been
associated with problems impacting health and economic, social and environmental
sustainability. Such activities compromise the population’s food and nutrition
security as well as its food sovereignty, and contribute to an unequal food system
that concentrates power and income in, and is highly dependent on, transnational
corporations.
Corporate political activity – a term used here to refer to ‘corporate attempts
to shape government policy in ways favorable to the rm’ (Mialon et al, 2015) –
contributes to this situation through various strategies including: nancial incentives
for political parties and decision-makers; promotion of certain messages (lobbying
decision-makers; promotion of deregulation); building favourable public opinion; and
use of legal means to block opponents and inuence trade agreements.
Such corporations are involved in situations where there are conicts of private and
public interests, and often rely on unethical means to defend their trade objectives.
In the international scenario, the degree to which conicts of interest are recognised
varies between countries. In Brazil it has received little attention and the issue is
not addressed explicitly either in the production and dissemination of information,
or in food and nutrition policies. Government eorts to regulate the private sector
have been insucient. Meanwhile, the sector’s strong and systematic resistance to
regulatory measures prevents progress on public policies.
In Brazil, the creation of FRRPPAN – Frente pela Regulação da Relação Público
Privado em Alimentação e Nutrição (Front for Regulation of the Public-Private
Relationship in Food and Nutrition) – a collective of researchers, professionals,
activists and policy-makers around political action to advance regulatory strategies,
has been essential for promoting the public agenda. Established in 2013 in a
favourable institutional political context, FRRPPAN’s political action is based on the
ethical principles of independence, autonomy, integrity, coherence and reliability. It
uses the following denitions: ‘public interest’ – the principles and values expressed
in public policies, in legal mechanisms for safeguarding and guaranteeing rights,
and in political action by collectives; ‘private sector’ – the economic agents that
act directly or indirectly in the area (in this case, in food and nutrition and the food
system) and that aim at prot (Castro, 2015); and ‘conict of interests’ – a situation
generated by a clash between public and private interests that can compromise the
collective interest or improperly inuence the performance of the public role (Castro,
2015).

48
Public health and the food and drinks industry: The governance and ethics of interactionCASE 4: Brazil
FRRPPAN’s political action has highlighted the following ethical issues:
• potential conicts of interest in the relationship between the private sector and
government institutions, and between the private sector and researchers or
research institutions; and
• issues related to companies’ production and political activities, that clash with the
public interest by compromising the health objectives and/or principles of public
policies, such as equity and social justice – for example, misleading advertising of
their products.
This case study analyses the political action of the collective, and initiatives inspired
by or related to its activities, highlighting strategies, advances, challenges, and the
factors inuencing such action.
Case
The action of the collective began at the World Nutrition Rio 2012 Congress. The
Congress, organised in total nancial independence of sectors with commercial
interests in the area of food and nutrition, expanded and extended the debate
on conicts of interest, and mobilised political action on this issue. A group of
scientic societies, professional associations, researchers and health professionals
then worked to develop the issue further. In 2013, this gave rise to the Frente pela
Regulação da Relação Público Privado em Alimentação e Nutrição (FRRPPAN).
Since then, FRRPPAN has:
• increased awareness of the conicts of interest issue in Brazil, identifying it as a
problem and putting it on the political agenda, by producing articles to publicise
concepts and arguments and to challenge conictive relationships that were
previously taken for granted (Castro, 2015; Frente pela Regulação da Relação
Público Privado em Alimentação e Nutrição, 2013; Burlandy et al, 2016; Gomes,
2015; Canella et al, 2015);
• promoted and participated in events, discussing the issues with dierent
audiences; and
• maintained a blog to support and publicise the Front’s activities (Blog da Frente
Pela Regulação da Relação Público Privado em Alimentação e Nutrição, 2017).
In 2014, a new space was created for networking and negotiation: the ‘Task Force
to Promote Bills of Law to Regulate Food Advertising, Labelling, and Environments’
(Força Tarefa para Avançar Projetos de Lei na Área da Regulação da Publicidade

49
Public health and the food and drinks industry: The governance and ethics of interaction CASE 4: Brazil
de Alimentos, Rotulagem, FTR in Portuguese), which brings together members
of civil society, government and academia with the aim of developing concerted
political action to advance the regulatory agenda. In 2016, which preceded the
coup in Brazil, the political dialogue between civil society and the government was
weakened. We maintained contact with the technical teams in the ministries, but by
2016 these teams had already been curtailed in their formal relationship with civil
society. As a result, we chose to reinforce more independent actions by civil society.
The experience with FRRPPAN and FTR contributed to the formation of a third
collective in 2016, Aliança pela Alimentação Adequada e Saudável – AAAS (Alliance
for Adequate and Healthy Eating) (Aliança pela Alimentação Adequada e Saudável,
2017), consisting of public interest civil society organisations, professionals,
associations and social movements. Its purpose is collective advocacy aimed
at greater political inuence in the area of food and nutrition, independent from
government and free of conicts of interest with the food industry.
Linkage between these three initiatives has allowed more incisive action in the
promotion and defence of regulatory restrictions on the promotion of unhealthy
food products and practices (e.g. advertising, labelling, sponsorships and prizes).
Examples include integrated action in public hearings on the Brazilian regulatory
agenda, and publicising situations of conicts of interest involving government
agencies and food companies (Vermelho Portal, 2012; World Public Health Nutrition
Association, 2011) and social activists and these companies (Associacão de
Agricultura Orgânica et al, 2016).
Eorts have also been made to develop mechanisms to safeguard against and
mitigate conicts of interest in academic institutions, including:
• workshops to promote reection on conicts of interest and produce backing for
developing a code of conduct for academic institutions
• creation of an advisory committee to support the administration and governance
of the Oce of the Director of the Institute of Nutrition at the Federal University of
Rio de Janeiro to provide guidance on principles for the procedure of analysis of
conduct involving public-private relations at this institution, and
• the Brazilian Association of Nutrition reviewing its sponsorship policy for events,
to include clear rules to limit participation by companies whose products
and practices are contrary to health and “adequate and healthy eating”. The
sponsorship policy was implemented at the 2016 Brazilian Congress of Nutrition,
and endorsed for use at future events (CONBRAN, 2016).
50
Public health and the food and drinks industry: The governance and ethics of interactionCASE 4: Brazil
Alternative scenario
Brazil’s current scenario diers signicantly from 2012, when the process described
in this case study began. We are now experiencing a profound economic and
political crisis, aggravated by the current administration’s decision to adopt a policy
of scal austerity, cutting funding to public universities, reducing investments in and
dismantling social policies, as well as politically undermining democratic arenas for
dialogue and cooperation between government and society.
In this scenario, there would be little possibility for knowledge-building and shared
political action among members of the collective, or for the capacity to inuence
existing decision-making circles. Thus the process described here would be limited
and would be unlikely to develop with any government support. The sustainability
of advances achieved so far will depend partly on the civil society organisations’
resilience and capacity for mobilisation in this process, and partly on their networking
with international stakeholders.
Discussion
Case questions
1 Why was the shared building of concepts essential for establishing a basis for political
action?
2 Why link different actors who act in different collective spaces?
3 Why invest in processes to formalise mechanisms for safeguarding against conflicts of
interest within academic institutions?
4 Which factors impacted on the advances and challenges?
The shared construction of ethical principles and concepts (as mentioned in the
Introduction) for analysing situations that involve public and private interests was
indispensable for producing minimum consensuses that oriented the development
of arguments and strategies for political action. This was essential given that, at the
beginning of this process, in Brazil, conicts of interest and other ethical dilemmas
in the public-private relationship had not previously been addressed in the food and
nutrition agenda.
The creation of dierent collectives happened as a function of: 1) the respective
motivations of the stakeholders; and 2) windows of opportunity and constraints
in the contexts that played out over the course of this process. While FRRPPAN
is dedicated to building and disseminating the discourse and arguments for the
regulatory agenda, FRT was dedicated to linking government experts and members

51
Public health and the food and drinks industry: The governance and ethics of interaction CASE 4: Brazil
of civil society in favour of specic regulatory projects at a time when the political
scenario tended to strengthen public policies in food and nutrition. Meanwhile, AAAS
has a representative constituency in various states of Brazil and has been able to
expand the scope of its activity by incorporating partners working on the food and
nutritional security agenda.
Brazil has incipient institutional mechanisms for dealing with conicts of interest and
other situations that violate ethical principles and the public interest. Given the prole
of the stakeholders involved in FRRPPAN (many of whom have university aliations),
we found that the collective construction of these mechanisms was an important
strategy for advancing the debate and practices in this area.
Factors that contributed to the advances were:
• government investment in universities and public policies
• civil society policy networks and mechanisms and structures for participatory
shared management and governance at the national level, and
• participation by researchers, activists and professionals in these spaces, building
alliances between these stakeholders and sectors of the federal government that
support the regulatory agenda.
Among the main challenges were:
• continuity in the process of understanding conicts of interest and other ethical
issues, and
• Brazil’s currently adverse political and economic context, which has had a major
impact on public policies and civil society action.
52
Public health and the food and drinks industry: The governance and ethics of interactionCASE 4: Brazil
Declarations of interests
Inês Rugani Ribeiro de Castro
None declared.
Camila Paes de Carvalho
None declared.
Paulo Castro Jr
None declared.
Luciene Burlandy
None declared.
Veruska Alexandre
None declared.
Ana Feldenheimer da Silva
Financial services:
Technical consultant to the World Bank to write a country case study on the strategies that Brazil has used to
control and prevent obesity.
Luciana Maldonado
None declared.
Daniela Canella
None declared.
References
Aliança pela Alimentação Adequada e Saudável (2017). http://www.alimentacaosaudavel.org.br/
Associacão de Agricultura Orgânica, Associacão Catarinense de Nutricão, ACT Promocão da Saúde, et al (2016). Open letter to chef
Jamie Oliver. http://actbr.org.br/uploads/conteudo/1093_CartaJO_ingles.pdf
Blog da Frente pela Regulação da Relação Público Privado em Alimentação e Nutrição (2017).
http://regulacaopublicoprivado.blogspot.com.br/
Burlandy L, Alexandre VP, Gomes FS, et al (2016). Health promotion policies and potential conflicts of interest involving the
commercial private sector.
Ciência e Saúde Coletiva
, 21: 1809-18.
Canella DS, Martins APB, Silva HFR, et al (2015). Food and beverage industries’ participation in health scientific events:
considerations on conflicts of interest.
Revista Panamericana de Salud Pública
, 38: 339-43.
http://www.scielosp.org/scielo.php?script=sci_arttext&pid=S1020-49892015000900011 [Accessed 12 October 2016.]
Castro IRR (2015). Relação público-privado, conflito de interesses e a agenda regulatória para a consolidação da democracia.
Ensaios e Diálogos em Saúde Coletiva, 1: 74-80.
CONBRAN (2016). Carta de Porto Alegre. http://www.asbran.org.br/arquivos/CARTA_PORTOALEGRE.pdf
Frente pela Regulação da Relação Público Privado em Alimentação e Nutrição (FRRPPAN) (2013). Manifesto de criação da Frente
pela Regulação da Relação Público-Privado em Alimentação e Nutrição.
http://regulacaopublicoprivado.blogspot.com.br/p/manifesto.html [Accessed 9 October 2016.]
Gomes FS (2015). Conflicts of interest in food and nutrition.
Cadernos de Saúde Pública
, 31 (10): 2039-46. http://www.scielo.br/
scielo.php?script=sci_arttext&pid=S0102-311X2015001002039&lng=en&nrm=iso [Accessed 10 October 2016.]
Mialon M, Swinburn B, Sacks G, et al (2015). A proposed approach to systematically identify and monitor the corporate political
activity of the food industry with respect to public health using publicly available information.
Obesity Review
, 16 (7): 519-30.
doi: 10.1111/obr.12289
Vermelho Portal (2012). Coca-Cola na campanha da Anvisa provoca nota de repúdio. 27 April 2012.
http://www.vermelho.org.br/noticia/181833-6
World Public Health Nutrition Association (2011). Brazilian health ministry burgered.
World Public Health Nutrition Association
,
June 2011. http://www.wphna.org/htdocs/2011_june_hp6_mcdonalds.htm
53
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
Summary
The Canadian government established two ministerial advisory committees –
the Trans Fat Task Force in 2004 and the Sodium Working Group in 2007 – to
address public health nutrition problems caused by unhealthful formulations of
food by food manufacturers. Each committee included 25 members – about
one-third each of representatives of government, health NGOs/researchers, and
industry.
The Trans Fat Task Force’s report, published in 2006, recommended that the
government introduce regulations limiting the permissible percentage-by-weight
of trans fat in dierent types of foods. One year later the government announced
that the food industry would be allowed an additional year to voluntarily reduce
trans fat levels before deciding whether even to begin consultations on draft
regulations. This was then followed by a decade of unexplained inaction, a
course from which Health Canada did not stray until after the 2015 general
election led to a government-wide change in political leadership.
The Sodium Working Group’s report, published in 2010, included 33 unanimous
recommendations and one majority recommendation which, if implemented,
would have protected one-to-two year-olds from restrictions on salty foods
that still only protect children under one year of age. In 2012, Health Canada
published voluntary sodium-reduction targets for 94 food categories consumed
by the general population, but these were largely ignored by food companies
and adherence was not publicly tracked by the federal government.
Unanimity or near-unanimity in both these reports may have stalled reforms
by misleadingly suggesting agreement among civil society, government and
industry, and thereby leading to complacency among health advocates.
Industry involvement in government nutrition
advisory groups in Canada: a decade of inaction
on trans fat and sodium
5
CASE
Author
Bill Jeffery
Executive Director,
Centre for Health
Science and Law,
Ottawa, Canada
Corresponding author
Bill Jeffery
Email: billjeffery@
healthscienceand
law.ca

54
Public health and the food and drinks industry: The governance and ethics of interactionCASE 5: Canada
Introduction
When governments appoint multi-stakeholder advisory bodies with weak conict-of-
interest safeguards, they court advice for ineectual, non-binding public health policy
measures (Lincoln et al, 2011; Conict of Interest Coalition, 2011, 2014; Centre for
Health Science and Law, 2016).
In the case of reducing trans fat and sodium in the Canadian food supply,
public opinion and the members of two relevant public-interest-mandated multi-
stakeholder committees – the Trans Fat Task Force and the Sodium Working Group
– solidly supported a strong government public health response. However, some
industry-oriented committee members were able to publicly back strong measures
while knowing that such support would not legally bind the food companies they
serve, nor preclude industry from lobbying government against introducing public
health regulations.
Providing advice to public health authorities is a public service that, in some ways,
is even more important than judging a courtroom dispute, enforcing most laws,
reporting news stories, providing medical care, or conducting scientic research,
because the duration and quality of thousands of lives are often impacted in
perpetuity by policies informed by government consultants. When the trust-holder
has a signicant competing private nancial interest, it should not be presumed to be
able to act contrary to that nancial interest. Having money in the game introduces
bias around the outcome.
Case
Trans Fat Task Force
Composition and inception
The Trans Fat Task Force was appointed in 2004 by the centrist Liberal Party’s
federal Minister of Health, following the passage of a non-binding House of
Commons resolution urging action. The Task Force had 25 members, consisting
of approximately one-third each of representatives of government, health
NGOs /researchers, and industry. There were seven food industry association
representatives, as well as representatives of at least two non-governmental
organisations that were known to rely on signicant funding and governance
involvement from food companies and industry associations (Dietitians of Canada,
and the now-defunct Canadian Council of Food and Nutrition), and a government
department that traditionally promotes the interests of the agriculture sector,
Agriculture and Agri-Food Canada.

55
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
Federal government and industry representatives tended to be senior, expert
professionals based in Ottawa and Toronto institutional headquarters with high
capacities for institutional support, while most public health representatives were
drawn from poorly resourced groups, or were issue generalists. The Minister of Health,
ultimately, selected the members on the advice of Health Canada bureaucrats.
Deliberations
When the Task Force began its deliberations in 2004, the Canadian food supply was
said to have the highest levels of trans fat in the world, causing an estimated 8,000
deaths per year. The Task Force held several public hearings in which expert and
industry witnesses were invited to give testimony and be questioned by Task Force
members. However, the Task Force did not have the power to compel witnesses to
testify and did not produce a verbatim transcript of the hearings or meetings.
The work of the Task Force culminated in the publication of its report to the Minister
of Health, TRANSforming the Food Supply, in 2006 (Trans Fat Task Force, 2006).
Just months after the Task Force published its report, the Liberal government was
replaced by a Conservative government that remained in power until 2015.
Recommendations
In its report, the Task Force recommended that the federal government use its
authority to promulgate, by 2008, regulations prohibiting the sale (by 2010) of fats
and oils containing more than 2% trans fat by weight, and multi-ingredient products
containing fats that are more than 5% trans fat by weight. (The larger percentage
for multi-ingredient products was due to the diculty of distinguishing articially
created trans fats from naturally occurring trans fats in dairy, beef and lamb.) Dietary
modelling by Health Canada scientists predicted that such regulations would
reduce the amount of trans fat in the food supply to a level that the World Health
Organization considers safe.
The multi-stakeholder agreement – illusory and politically misleading
Importantly, the nal Task Force recommendations were publicly supported
unanimously by its 25 members. However, in 2007, just one year after the
publication of the Task Force report, the Conservative Minister of Health announced
on behalf of the government of Canada that the food industry would be allowed
one additional year to voluntarily reduce trans fat levels before deciding whether
even to begin consultations on draft regulations, thereby delaying the Task Force’s
timeline by two years. The delay was immediately welcomed by Task Force member
the Canadian Restaurant and Foodservice Association (later renamed Restaurants
Canada), which had previously endorsed the original timeline for regulations
(Canadian Restaurant and Foodservices Association, 2007).

56
Public health and the food and drinks industry: The governance and ethics of interactionCASE 5: Canada
Unanimity in the Trans Fat Task Force report may have stalled reforms by
misleadingly suggesting agreement among civil society, government, and industry
and thereby leading to complacency among health advocates.
The politicians (e.g. the Prime Minister, Minister of Health, and Parliamentary Secretary
to the Minister of Health in the Conservative government) were persistently ambiguous
about the extent of their support for the unanimous recommendations. Industry-
aliated Task Force members would not be likely to provide full support for new
public health regulations that could cost their benefactors many millions of dollars
in implementation costs, lost prots, regulatory penalties, or public embarrassment.
Also, importantly, industry associations are voluntary in nature and do not have the
legal authority to bind member companies, so their purported commitment is more
of a public relations gesture than a warranty of future performance.
What has happened since the publication of the Task Force report?
While there are encouraging indications that trans fat levels in the Canadian food
supply have declined in recent years under the lingering threat of regulation, Health
Canada has not yet published comprehensive data since cancelling the Trans Fat
Monitoring Program in 2009. The publication of the Trans Fat Task Force report in
2006 coincided with the beginning of a decade of inaction on public health nutrition
in Canada. It was later revealed that, in 2009, Health Canada had cancelled the
Trans Fat Monitoring Program and derailed eorts to restrict the use of partially
hydrogenated oils (Schmidt, 2012).
The next government, which came into power in 2015, did make good on its
election platform commitment to ban partially hydrogenated oils by adding them to
the List of Contaminants and Other Adulterating Substances in Foods (Government
of Canada, 2017).
Sodium Working Group
Composition and inception
Health Canada began to take note of the need to reduce sodium in the Canadian
food supply shortly after the publication in 2006 of a World Health Organization
expert report – Reducing Salt Intake in Populations – which called on member states
to act (World Health Organization, 2007). In 2007, shortly after a cadre of Canadian
health organisations called on the federal government to heed the WHO report,
the federal Minister of Health appointed the 25-member Sodium Working Group
– comprised of approximately one-third each of industry, government, and health
researchers/advocates – to advise on a government response.

57
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
Deliberations
From 2008 to 2010, the Sodium Working Group followed the same general operating
procedures as the Trans Fat Task Force had in 2004-2006. The Sodium Working
Group
advised the Minister of Health directly in its report
Sodium Reduction Strategy
for Canada
(Sodium Working Group, 2010), after which the Group was unceremoniously
disbanded by a teleconference message delivered by the Health Canada sta
representative on the Group (House of Commons Standing Committee on Health, 2011).
Recommendations
In its report, the Sodium Working Group made 33 unanimous recommendations,
including recommendations to mandate reforms to food labelling, restrict marketing
to children, and monitor voluntary, time-delimited sodium reduction eorts by
industry. There was also one majority recommendation to set regulatory limits
on sodium levels in foods marketed to toddlers. These recommendations were
designed to aid the pursuit of voluntary sodium reduction targets which modelling
forecasts indicated would be enough to reduce population sodium levels by
approximately 32% within ve years.
The multi-stakeholder agreement – illusory and politically misleading
In 2012, Health Canada published voluntary sodium-reduction targets for 94 food
categories, but these were largely ignored by food companies and adherence
was not publicly tracked by the federal government. (However, a comprehensive
assessment is expected to be published.)
In 2013, after three years of inaction on the recommendations of the Sodium
Working Group, a vote was held on legislation – proposed by an opposition party
Member of Parliament – which would have mandated implementation of the
strategy. The legislation received unanimous support from opposition MPs from all
parties and one vote from the governing Conservative party, but was defeated by
the Conservative majority in the House of Commons. The 2013 annual report of
the leading pre-packaged food industry association, Food and Consumer Products
of Canada (FCPC), took credit for defeating the bill, stating: “FCPC launched a
pro-active campaign to ensure an NDP sodium bill, which called for misguided
regulations and sodium warning labels on products, was defeated.” (Food and
Consumer Products of Canada, 2013).
The importance of measuring progress with public health purpose
It is important to set quantiable benchmarks against which progress is easily
measured. The European Platform for Action on Diet, Physical Activity and Health
reported industry-supplied progress measures without putting them in context.

58
Public health and the food and drinks industry: The governance and ethics of interactionCASE 5: Canada
Humans collectively consume billions of tons of food annually, so boasting the
removal of 822 tons of salt from the European food supply, as noted in the European
Platform in 2008, was in fact only a reduction of approximately 1/100th of 1% of
baseline salt intake at a time when 30%-50% reductions were advised by public
health experts.
1
On that trajectory, if the comparatively tiny average reduction
during the Platform reporting period were repeated annually through successive
reductions into the future, it would take an estimated 4,443 years to reduce sodium
from approximately 4,000mg (10 grams of salt) per capita per day to the 2,000mg
(5 grams) recommended by the World Health Organization. The European Platform
for Action on Diet, Physical Activity and Health consists of 34 members, nearly half
of whom represent Europe’s largest, multi-billion-euro food, beverage and media
companies and several health groups that were signicantly funded by food and
pharmaceutical companies.
Health Canada decided to establish targets and gauge progress toward achieving
sodium-reduction goals by measuring sales-weighted averages for product
categories. However, charting progress against this metric requires purchasing
expensive industry-wide sales data and does not x responsibility squarely on
the shoulders of companies or individual products. This is likely to mean that
only government or very well-funded academic researchers can verify industry
compliance, and that no companies or products would be blameworthy for
excessive saltiness. If sodium-reduction targets were based on absolute levels
in food categories, and companies were required to disclose levels to a publicly
accessible database, consumers and researchers could easily track progress and
best hold companies to account.
In October 2016, at a Health Canada ‘Symposium on Sodium Reduction in Foods’
– convened under the political leadership of the new Liberal government – Food and
Consumer Products of Canada (the largest food industry association) reported that
“6 of 9 categories of foods surveyed by Health Canada achieved signicant sodium
reduction.” (Food and Consumer Products of Canada, 2016). However, Health
Canada reported that, in its review of sodium levels in 1,000 foods in 2009 and
2016, only one of 15 categories achieved Health Canada’s sodium reduction targets
and, even in that category, the sample of foods was too small to make reliable
inferences about actual changes. In the sample for one category, packaged deli
meats, there was actually a small increase in sodium levels (Kuran, 2016).
1
EU Platform on Diet, Physical Activity and Health Annual Report 2008
states: “Figures provided to the Platform suggest that Members have removed at least 822 tonnes of
salt from food products since 2004.” (EU Platform on Diet, Physical Activity and Health, 2008). However, 500 million Europeans consuming only the WHO-recommended 5g
of salt daily would have consumed approximately 3.65 million tons of salt during the 4-year period. (5 grams/person-day X 365 days/year X 4 years X 500 million people,
divided by 1,000,000 [1,000,000g = 1 ton].) Considering that many Europeans consume nearly double WHO recommended intake, this constitutes as little as 1/100th of 1%
of current intake, an undetectable rounding error. Furthermore, some of the pledges were for world-wide operations (not just Europe), so the contribution to public health is
even more diffuse to the point of being imperceptible, and far from boast-worthy.
59
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
Political will to implement public health measures
During the 2015 general federal election, the opposition Liberal Party campaigned
partly on a promise to “bring in tougher regulations to eliminate trans fats, similar to
those in the U.S., and to reduce salt in processed foods” (Liberal Party of Canada,
2015). The implementation failures of the Sodium Working Group and Trans Fat Task
Force and on-going media coverage of those failures undoubtedly played a role in
inspiring the new government’s election platform commitments, the obligations to
address trans fat and sodium in the Prime Minister’s published ‘Mandate Letter’ to
the Minister of Health in 2015 (Trudeau, 2015), and in the Minister’s announcement
of her
Healthy Eating Strategy
in October 2016 (Health Canada, 2016).
Alternative scenario
If the Sodium Working Group had been truly independent of industry and had
remained intact to monitor implementation, it could have published challenging
progress reports, and its authoritative position as the key external advisory body
to the Minister on sodium reduction could have helped engender compliance by
industry.
Discussion
Case questions
1 Should representatives of the food and drinks industry be included, and have decision-
making powers, in nutrition advisory panels? Or should their role be as witnesses to
appear before an independent advisory panel?
2 Many public servants have to sign an oath of confidentiality. What effect does this have
on government transparency?
3 What other ways are there to limit the influence of industry on government?
1 Should representatives of the food and drinks industry be included, and have
decision-making powers, in nutrition advisory panels? Or should their role be as
witnesses to appear before an independent advisory panel?
Industry-aliated members of advisory groups are motivated to steer health policy
advice towards ineectual voluntary measures, and even to make proclamations of
support for strong public health measures. However, industry associations have no
authority to bind their member companies to be good public health actors, and also
companies remain free to lobby discreetly against regulations. Companies’ nancial
incentives and legal duties to shareholders trump nebulous and contestable moral
responsibilities to protect health.

60
Public health and the food and drinks industry: The governance and ethics of interactionCASE 5: Canada
In both cases – trans fat and sodium – no federal regulations were promulgated
by government in the ten and six years, respectively, that followed publication of
the Minister-commissioned advice. (In September 2017, the federal government
nalised its decision to revoke the regulatory approval of partially hydrogenated oils,
to become eective on 13 September 2018.)
Governments sometimes need to tackle complex public health nutrition problems
that demand nuanced, coherent advice based on fresh perspectives. Appointing
non-governmental parties, especially knowledgeable opinion-leaders among
university academics, non-governmental public interest groups, and other levels of
government to limited-term advisory committees can oer governments exible,
informed, comprehensive and coherent advice. While input from industry can be
useful, there is a moral hazard that industry advice and information will be tailored
to suit the commercial purposes of its proponents. Representatives of companies,
trade associations, and industry-funded non-governmental organisations should be
invited as witnesses (not panel members) to appear before independent advisory
panels, in circumstances where they can be cross-examined by panel members.
Parties with nancial stakes in food, drug, and medical technology, and other
companies, should not be invited to have continuing roles on advisory committees.
The moral hazard is too great that committee members with nancial conicts of
interest would steer other committee members away from eective policy solutions,
disrupt consensus, promote weak compliance measures, or feign support for
consensus recommendations while discreetly opposing strong tax and regulatory
measures outside the group.
The World Health Assembly recently conferred considerable discretion on the World
Health Organization to establish regulatory safeguards to govern these high-risk
relationships (Garde, et al, 2017; Centre for Health Science and Law, 2016). These
safeguards should caution governments against appointing commercially motivated
nutrition advisors.
2 Many public servants have to sign an oath of condentiality. What eect does this
have on government transparency?
It is challenging to make condent inferences about the precipitants of government
decisions, partly because public decision-making is complex, with many parties and
types of information playing inuential roles. Also, public servants are contractually
sworn and institutionally encouraged not to reveal certain internal government
deliberations and to serve their bureaucratic and political masters with loyalty
(Supreme Court of Canada, 1985). Cabinet ministers take life-long oaths not to
divulge certain information, and less protected oral and written communications

61
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
among lobbyists and other government ocials are rarely proactively disclosed to
the public (Supreme Court of Canada, 2002; Governor General of Canada, 2015).
For example, Health Canada documents obtained via an Access to Information Act
disclosure seemed to reveal that a decision had been taken by the Minister of Health
in 2009 to promulgate regulations to ban the use of partially hydrogenated oil, but
that course of action was abruptly halted by the Prime Minister’s Oce. However,
the available public record is not unequivocal on this point, perhaps due to the
reluctance of government ocials to be seen to be reecting in writing an unpopular
decision that the government is inclined to keep secret for political advantage.
Whistle-blower protections for Canadian federal public servants are considered
weak, with vocal critics risking their employment being terminated (Federal Court of
Canada, 2014).
The resulting lack of clarity of the public record makes causal attribution (not
to mention public accountability and measuring progress) dicult, especially in
disentangling the potential inuence of the food industry from the shift from a
politically conservative government to a more activist government. While the current
government has not reinstated the Sodium Working Group, it has substantially
implemented the recommendations of the Trans Fat Task Force as it committed
to do in its election platform, the Health Minister’s Mandate Letter, and the
Healthy
Eating Strategy
to promulgate binding regulations to lower sodium levels in foods –
one step further than the Sodium Working Group advised in 2010.
3 What other ways are there to limit the inuence of industry on government?
• Preventing election candidates from accepting nancial contributions from industry
It is likely to be benecial for public health that candidates for election to the
federal House of Commons and several provincial legislatures be forbidden
from accepting nancial contributions from any type of corporation. Allegations
that industry successfully pressured government to thwart public health infers
corruption which, in Canada, could be prosecuted under a rarely-enforced
section of the Criminal Code (Frauds on the Government), and punishable by
imprisonment of up to ve years. Threats by industry to government – for example,
of capital ight (moving manufacturing plants o-shore to avoid regulations) – are
hard to prove and rarely declared publicly.
• Allowing public health advocates and charities to be vocal on public health issues
It is potentially important that the current government won oce on an election
platform that included proposals to promulgate regulations to reduce sodium
and trans fat. In future elections, key public health advocates may be free to be
62
Public health and the food and drinks industry: The governance and ethics of interactionCASE 5: Canada
more vocal on these and other public health issues, and the same may apply to
all charities if the federal government fulls its election platform commitment in a
manner that comports with the advice from its own expert panel (Consultation
Panel on the Political Activities of Charities, 2017). For decades, and especially
in recent years, health charities have been reticent to speak publicly about health
policy during and even between elections, for fear of having their charitable tax
status revoked by very arcane and constrictive charity regulations. Private sector
companies have much looser restrictions on lobbying and media communications
about public policy issues compared to the rules currently applied to charities.
Declarations of interests
Bill Jeffery
None declared.
References
Canadian Restaurant and Foodservices Association (2007). Foodservice industry applauds Minister of Health for action on trans fat. Media
comment. 20 June 2007. http://www.newswire.ca/news-releases/foodservice-industry-applauds-minister-of-health-for-action-on-trans-
fat-533895211.html
Centre for Health Science and Law (2016). Media statement. World Health Organization weakens conflict of interest safeguards. 28 May
2016. http://healthscienceandlaw.ca/wp-content/uploads/2016/06/WHO.Critique.Conflicts-of-Interest.pdf
Conflict of Interest Coalition (2011). Statement of Concern published at the United Nations General Assembly meeting in New York City in
September 2011 (endorsed by 160 groups and networks, representing more than 2,000 non-profit associations internationally).
http://healthscienceandlaw.ca/wp-content/uploads/2016/09/conflict-of-interest.2011Statement.pdf
Conflict of Interest Coalition (2014). Statement of Concern published at the United Nations General Assembly meeting in New York City in
July 2014 (endorsed by 175 groups and networks, representing more than 2,000 non-profit associations internationally).
http://healthscienceandlaw.ca/wp-content/uploads/2016/10/UN.Conflict-of-interest-safeguards.Health-trump-trade.July2014.pdf
Consultation Panel on the Political Activities of Charities (2017).
Report of the Consultation Panel on the Political Activities of Charities,
March 31, 2017
. Canada Revenue Agency. http://www.cra-arc.gc.ca/chrts-gvng/chrts/cmmnctn/pltcl-ctvts/pnlrprt-eng.html
EU Platform on Diet, Physical Activity and Health (2008).
EU Platform on Diet, Physical Activity and Health: Annual Report 2008
.
http://ec.europa.eu/health/ph_determinants/life_style/nutrition/platform/docs/eu_platform_2008frep_en.pdf
Federal Court of Canada (2014). Shiv Chopra v. Attorney General. Chopra v. Canada (Attorney General), 2014 Federal Court of Appeal 179.
http://canlii.ca/t/gdrlh. Leave to appeal to the Supreme Court of Canada dismissed on July 14, 2015. Case No. 36091.
Food and Consumer Products of Canada (2013).
Insights, Interactions, Influence: Proudly Serving Canada’s Food and Consumer Products
Manufacturers for Over 50 Years
. Toronto at 8. http://www.fcpc.ca/Userfiles/FCPCReports/2013Secure/FCPCAMR13-Eng-Fn.pdf
Food and Consumer Products of Canada (2016). Michi Furuya Chang. Presentation to Health Canada’s Ottawa Symposium on Sodium
Reduction in Foods: Progress, complexity and choice: sodium reduction in the Canadian manufactured food supply.
Garde A, Jeffery B, Rigby N (2017). Implementing the WHO recommendations whilst avoiding real, perceived or potential conflicts of
interest.
European Journal of Risk Regulation
, 8: 237-50.
Government of Canada (2017). List of Contaminants and Other Adulterating Substances in Foods. https://www.canada.ca/en/health-
canada/services/food-nutrition/food-safety/chemical-contaminants/contaminants-adulterating-substances-foods.html
Governor General of Canada (2015). Oath of Office to which Canadian Cabinet Minister’s must swear or affirm their allegiance.
http://www.gg.ca/document.aspx?id=316
Health Canada (2016).
Healthy Eating Strategy
. https://www.canada.ca/content/dam/canada/health-canada/migration/publications/eating-
nutrition/healthy-eating-strategy-canada-strategie-saine-alimentation/alt/pub-eng.pdf
House of Commons Standing Committee on Health (2011). Testimony of Bill Jeffery, member of the Sodium Working Group. Evidence
(Transcript). No. 47, 3rd Session, 40th Parliament. February 3, 2011. Chair, Joy Smith.
http://www.ourcommons.ca/Content/Committee/403/HESA/Evidence/EV4928518/HESAEV47-E.PDF

63
Public health and the food and drinks industry: The governance and ethics of interaction CASE 5: Canada
Kuran C (2016). Presentation to Health Canada’s Ottawa Symposium on Sodium Reduction in Foods: Health Canada’s sodium monitoring
activities.
Liberal Party of Canada (2015).
Real Change: A New Plan for a Strong Middle Class Election Platform:
p20.
https://www.liberal.ca/files/2015/10/New-plan-for-a-strong-middle-class.pdf
Lincoln P, Rundall P, Jeffery B, et al (2011). Conflicts of interest and the UN high-level meeting on non-communicable diseases.
The
Lancet
, 378: e6. http://www.thelancet.com/pdfs/journals/lancet/PIIS0140-6736(11)61463-3.pdf
Schmidt S (2012). Health Minister nixed plan to limit trans fat in food, records show.
The Ottawa Citizen
, 6 February 2012, and records on
file with author.
Sodium Working Group (2010).
Sodium Reduction Strategy for Canada
. Ottawa: Health Canada.
http://www.hc-sc.gc.ca/fn-an/alt_formats/pdf/nutrition/sodium/strateg/reduct-strat-eng.pdf
Supreme Court of Canada (1985). Fraser v. Public Service Staff Relations Board, [1985] 2 Supreme Court Reports 455.
Supreme Court of Canada (2002). Babcock v. Canada (Attorney General) [2002] 3 Supreme Court Reports 3.
Trans Fat Task Force (2006).
TRANSforming the Food Supply
. Ottawa: Health Canada.
Trudeau J (2015). Mandate Letter to Minister of Health Jane Philpott.
World Health Organization (2007).
Reducing Salt Intake in Populations. Report of a WHO Forum and Technical Meeting 5-7 October 2006,
Paris, France
. http://www.who.int/dietphysicalactivity/Salt_Report_VC_april07.pdf
64
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Authors
Sebastián Peña
National Institute for
Health and Welfare,
Finland
Frente por un Chile
Saludable
Cecilia Castillo
Frente por un Chile
Saludable
Cristóbal Cuadrado
Programa de
Políticas, Sistemas
y Gestión en Salud,
Escuela de Salud
Pública, University
of Chile
María Teresa
Valenzuela
Escuela de Salud
Pública, University
of Chile
Frente por un Chile
Saludable
Corresponding
author
Sebastián Peña
Email: spenafajuri@
gmail.com
Summary
A crucial strategy of the food industry has been to interact with public
institutions, such as universities and public health institutes, in order to inuence
research and promote industry interests in the public debate. Facing severe
nancial constraints, some public universities in Chile have relied on funding
from the food industry to support research and project development. There is
a potential risk that these public-private partnerships may allow commercial
interests to bias research and permeate policy-making and public opinion.
This case study examines the long-standing relationship between the food
industry and the Institute of Nutrition and Food Technology (INTA) of the
University of Chile – the most prestigious food and nutrition-related institution
in the country. The types of collaboration include: industry-funded research,
scholarships and awards; membership of industry-funded or linked foundations;
awarding of nutrient-specic certication of foods that are high in calories,
sugar, saturated fats or salt; joint public health programmes; and marketing in
institutional publications and websites.
INTA plays a major role in food policy-making in Chile. Although it is unclear
whether the potential for conicts of interest arising from the relationship
between INTA and the food industry have inuenced policy-making, INTA’s
institutional mandate to conduct independent, high-quality research and
educational activities runs the risk of being compromised. The existence of
strong nancial ties between INTA and the food and drinks industry represents
a conict of interest, potentially compromising INTA’s independence in highly
relevant research and policy areas.
Food industry permeating public institutions:
the case of the Chilean Institute of Nutrition and
Food Technology
6
CASE

65
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Introduction
Latin America is currently facing an obesity epidemic and a large burden of disease
arising from non-communicable diseases (NCDs). Several countries in the region
are taking steps to implement policies to reduce obesity and NCDs (Pan American
Health Organization, 2015), such as taxes on sugar-sweetened beverages in Mexico
and Chile, and front-of-package labelling policies in Ecuador and Chile (International
Food Policy Research Institute, 2016; Fraser, 2013). The food industry has strongly
challenged regulation using media, lobbying and opinion leaders (Barquera et al, 2013).
A strategy of the food industry has been to collaborate with public institutions,
such as universities and public health institutes, in order to inuence research and
promote industry interests in the public debate (Nestle, 2016). These partnerships
have been extensively documented in the United States and Canada and have
extended to Latin America (Moodie et al, 2013; Freedho and Hebert, 2011;
Monteiro and Cannon, 2012).
In Chile, academic institutions have an important role in generating knowledge and
providing expert support for food and nutrition policy. As some of them have relied
on funding from the food industry to support research and project development,
there is a risk that these public-private partnerships may allow commercial interests
to bias research and permeate policy-making and public opinion.
This case study aims to describe the relationship between an academic institution
and the food industry, analyse ethical challenges arising from this relationship, and
suggest strategies to address conicts of interest. For this purpose, we examine the
15-year old relationship between the food industry and the Institute of Nutrition and
Food Technology (INTA) of the University of Chile, the most prestigious food and
nutrition-related institution in the country.
We systematically searched the INTA website, including the information on contracts
and collaboration agreements published as a requirement of the Transparency Law
(Law 20.285/2008). Using the Transparency Law, we requested detailed information
from INTA on contracts and collaboration agreements from 2005 to 2016. We
also analysed documents published by INTA, extracting information about industry
marketing and news about industry collaboration. Industry marketing was dened
as any mention of commercial products or brands in advertising or direct coverage
of an industry product within an article published by INTA on their website. We then
expanded the review to include websites of commercial organisations and other
academic institutions mentioned on INTA’s website. The information on collaboration
agreements obtained under the Transparency Law can be found in in Table 1 on
page 74.

66
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Case
In its Institutional Development Plan 2015-2025, the Institute of Nutrition and
Food Technology of the University of Chile (INTA) states that it aims to promote
the creation of transdisciplinary knowledge, development of human capital and
knowledge transfer to society, contributing to optimal nutrition, health and quality
of life of the Chilean and Latin American population. Through these three areas
(research, training and knowledge transfer), INTA strives to become a “valid
interlocutor with other actors to tackle the NCDs and obesity epidemic, such as the
State, industry and civil society. This implies promoting these interactions, but also
establishing transparent evaluation mechanisms that allow safeguarding the ethical
and intellectual independency of INTA” (Instituto de Nutrición y Tecnología de los
Alimentos, 2016b).
INTA plays a major role in food policy-making. It is a regular member of the
Advisory Committee for the Revision and Update of the Sanitary Regulation Code
(Decree 977/1996) and participated in the ad hoc commission that dened the
current Decree for the Food Labelling Law. INTA also has a consultancy rm that
participates in public bids to carry out research. For example, in 2011 the Ministry of
Health commissioned INTA to carry out a study to establish the nutrient limits for the
Food Labelling Law.
We identied various types of collaboration between INTA and the food industry
from 2002 to 2016 including: industry-funded research, scholarships and awards;
membership of industry-funded or linked foundations; nutrient-specic certication
of foods that are high in calories, sugar, saturated fats or salt; joint public health
programmes; and marketing in institutional publications and websites.
Industry-funded research, scholarships and awards
Research collaboration dates back to at least 2002, when INTA developed a
partnership with Tresmontes Lucchetti, a large producer of snacks, powder juices
and pasta. From 2002 to 2009, Tresmontes Lucchetti provided around $US 324,000
to carry out an obesity-reduction intervention in rural schools in Casablanca and
later on in an urban setting in Macul (Vio del Rio, 2012). INTA has also published
studies based on research funded by Nestlé, Danone and Benexia (Cruchet et
al, 2016; Fisberg et al, 2016; Valenzuela et al, 2015). However, it is worth noting
that INTA also receives a large amount of funding from national and international
research funds – including national funding from the National Health Fund (FONIS)
and the National Fund for Scientic and Technological Development (FONDECYT),
together with international funding from institutions such as the National Institutes of
Health in the US and the International Development Research Centre in Canada –

67
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
and, overall, funding from public institutions appears to greatly exceed the nancial
contributions from the food industry.
We found that the food industry also makes contributions to INTA in the form of
scholarships and awards – for example: the Dr Abraham Stekel Scholarship, for four
postgraduate scholarships to “contribute to the development of young professionals
carrying out research in INTA”, funded by Nestlé since 1988 (Nestlé, 2015a); and the
Dr José Manuel Celedón scholarship, awarded annually to four or ve postgraduate
students on INTA’s Masters Programme in Food and Nutrition, and funded by DSM
Nutritional Products, Chilean Poultry Producers and (in some years) Coca-Cola
(Instituto de Nutrición y Tecnología de los Alimentos, 2012; 2014).
Researchers from INTA have also been awarded the Henri Nestlé Award for scientic
research on nutrition six times, totalling 50% of all awards in nutrition since 2005
(Nestlé, 2014a). This industry award is given jointly with a scientic society: the
Chilean Society for Nutrition, Bromatology and Toxicology. INTA researchers have
also been members of the jury for the prize (Nestlé, 2014b).
No information was available on the role of the food industry in the design and
implementation of the research, nor on the selection of the scholarship recipients.
Membership of industry-funded or linked foundations
We found that several academics from INTA are listed as board members in
industry-funded or linked foundations. Most notable is the South-Andean section
of the International Life Sciences Institute (ILSI), funded by Unilever, Tresmontes
Lucchetti, Monsanto, Nestlé, Kraft, Danisco-Dupont, DSM and Coca-Cola (ILSI
Sur Andino, 2016). INTA researchers also received awards in 2015 and 2016 to
participate in the ILSI Annual Meeting (Instituto de Nutrición y Tecnología de los
Alimentos, 2015; 2016c). One researcher serves as a member of the Danone
International Institute and Director of Southern Cone and has been scientic adviser
for Unilever, Kraft, Knowles and Bolton, DSM and Kellogg’s (Instituto Danone Cono
Sur, 2016; Uauy et al, 2009).
Some INTA researchers are renowned experts in Latin America and worldwide
and have taken international leadership positions, including the presidency of the
International Union of Nutritional Sciences and the International Nutrition Foundation.
In both cases, this has entailed partnership agreements and fellowships with the
food industry, expanding the industry ties globally (International Union of Nutritional
Sciences, 2009; International Nutrition Foundation, 2012).

68
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Nutrient-specific certification of foods that are high in calories, sugar, saturated fats or salt
INTA is legally allowed (but not mandated) to provide certication of food products.
Prior to the implementation of the Food Labelling Law, INTA had certied over 25
food or alcohol products (Salt Lobos, Tresmontes Lucchetti, Surlat, Carozzi, CIAL,
Arcor and Cambiaso, Cooperativa Agrícola Pisco Elqui) (Instituto de Nutrición
y Tecnología de los Alimentos, 2013; Dirección de Asistencia Técnica, 2016). It
provided certication for specic nutrients (such as cacao content or gluten-free)
in otherwise energy-dense, nutrient-poor products. Certication, which includes
INTA’s logo, has appeared on the front of packaging, thus using INTA’s reputation
to promote unhealthy food. Since the implementation of the Food Labelling Law
in 2016, INTA has provided nutrient certication only to food products that are
classied as not high in calories, salt, sugar or saturated fat according to the nutrient
prole in the Food Labelling Law.
INTA also oers technical assistance to the food industry, including on food
labelling, health claims, nutrients and food regulation. Clients of these services
include Unilever, Bimbo Group, Nestlé, Danone, Soprole and Carozzi (Dirección
de Asistencia Técnica, 2016). INTA also oers food analysis for the food industry
(Dirección de Asistencia Técnica, 2016).
Joint public health programmes
The initial research collaboration between INTA and Tresmontes Lucchetti led
to an intervention called Healthy Space (Espacio Saludable), a programme for
the prevention and control of obesity and overweight in public schools, which
has expanded from the pilot to several municipalities (Kain et al, 2012; Espacio
Saludable, 2016). Another collaborative intervention is the Schools of Wellbeing
(Escuelas de Bienestar) programme, implemented with the Pontical Catholic
University, ILSI South Andean and the Coca-Cola Foundation, carried out in nine
public schools and involving 3,000 students (La Tercera, 2008; Bolumburu, 2010).
Since 2009, INTA and Nestlé have implemented the Children in Action (Niños en
Acción) programme, a collaboration with local governments to promote healthy
behaviours in schools. In 2016, the programme covered 40,864 children in schools
from 50 municipalities (Nestlé, 2016). This is part of a global initiative by Nestlé – the
Healthy Kids Programme – where Nestlé partners with the EPODE international
network for its global implementation of the programme (Nestlé, 2015b). (See Case 12.)
Since 2011, INTA, the School of Engineering of the Pontical Catholic University and
Nestlé launched the Platform for Food Innovation that organises a yearly Diploma in
Food Innovation (Plataforma de Innovación en Alimentos, 2016).

69
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Marketing in institutional publications and websites
Nutrition and Life, a bimonthly magazine published by INTA from 2012 to 2015,
featured food industry marketing in 13 out of 14 editions (93%). (See Table 2 on
page 76.) The most frequent partners have been Nestlé, Recalcine (probiotics) and
Wyeth (milk formula). In 2016, the magazine was converted to a website with blog
entries and contains marketing of Nestlé, Axon-Pharma and Recalcine, all featuring
products containing probiotics (Instituto de Nutrición y Tecnología de los Alimentos,
2016a).
INTA’s interactions with the food industry
Figure 1 provides a summary of INTA’s interactions with the food industry.
Whether the conicts of interest of INTA with the food industry have been able to
inuence policy-making is still unclear and remains a key area for further research.
Key
1 = Research funding, scholarships and awards
2 = Membership of industry-funded institutions
3 = Certification of products and technical assistance
4 = Implementation of public health programmes
5 = Marketing
Figure 1. Network of INTA’s links with the food industry, 2002-2017
Note to Sally - this Figure title was in last PD
70
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Discussion
Case questions
1 Why is it possible for a public institution like INTA to develop such a strong connection
with the food industry, potentially compromising its independence?
2 What measures can be taken to prevent commercial interests from influencing research
and permeating policy-making and public opinion?
The research-industry relationships are not new and their potential harmful eects
are well known (Katan, 2007; Bes-Rastrollo et al, 2013; PLoS Medicine Editors,
2012; Kearns et al, 2016; Nestle, 2013). However, both researchers and universities
have been reluctant to take formal action to reduce these types of interactions.
In this context, it is important to highlight that the mandate to a public research
university, such as the University of Chile, is to conduct independent, high-quality
research and educational activities, supporting the implementation of clinical
and policy innovation to increase societal wellbeing. Such a mandate represents
an agent-principal relationship, where the public and the government trust in
an agent (the university) to full very specic actions in the best interest of the
principal (society). When another principal with conicting interests, such as the
ultra-processed food industry, uses the university as an agent, there is a clear risk
of deviation from the primary societal mandate of the agent. Conicts of interest
arise when there is a risk of undue inuences (“risk that the professional judgment
or actions regarding a primary interest will be unduly inuenced by a secondary
interest”) (Institute of Medicine, 2009).
This case study raises important questions about the extent to which INTA may
have compromised its institutional mandate to promote research, training and
knowledge transfer by establishing a systematic and long-lasting partnership with
the food industry. The existence of strong nancial ties between INTA and the
industry arguably represents a conict of interest, potentially compromising INTA’s
independence in highly relevant policy areas. The ethical challenges arising from this
relationship may compromise both INTA’s integrity as a public institution, and the
individual professional integrity of those researchers involved in carrying out industry-
funded research and serving on the governing boards of food industry organisations.
Joint public health programmes, marketing on institutional websites and certication
of unhealthy food products are disturbing examples of the food industry taking
advantage of society’s trust in public institutions to improve their own public
image. The population receives contradictory messages from actors with opposing
agendas.

71
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Financial ties in the form of industry-funded research, certication and technical
assistance may constrain the necessary independent and free-of-bias expert opinion
of INTA in the policy-making processes in which it plays a key role (Freedho and
Hebert, 2011). It also risks indirectly providing the food industry with a seat at the
policy-making table. Indirect contributions in the form of scholarships and awards
can be subtle strategies on the part of industry to establish a trust relationship
between the industry and promising students and senior researchers, with the
potential to develop a continuum of inuence throughout their careers.
This case study also raises questions about the adequacy of safeguarding
mechanisms to prevent conicts of interest within the organisation, even though
this is stated in their Institutional Development Plan 2015-2025. It also shows
the weakness of public institutions such as the Ministry of Health and Ministry of
Education, as there are no formal mechanisms in Chile for the early detection and
prevention of the potential harmful eects of such conicts in the protection of the
public interest.
Only in the last few years has civil society begun to raise awareness of the ethical
and policy challenges of such conicts of interest. Since 2014, the Frente por
un Chile Saludable, a coalition of NGOs and civil servants, has started to draw
attention to these issues. In 2016, a social media campaign organised by concerned
professionals requested the Chilean Society of Pediatrics to stop receiving funding
from Coca-Cola. After much pressure, the Society ended the collaboration,
representing arguably the rst example of successful civil society pressure against
food-industry funding in Chile (Dominguez, 2016).
A key message of this case study is the need to prevent conicts of interest as
much as possible. This requires concerted action from research institutions and
researchers. To protect the public interest, governments need to promote deeper
evaluation and take clear action to prevent these situations. Academia and
top national research institutions are usually key advisors to governments, and
conicts of interest can have potentially harmful consequences for decision-making
processes. Protecting these policy spaces from indirect and direct industry inuence
is an important challenge for policy-making in modern democracies, particularly in a
context where trust in public institutions is diminishing or lacking (Papadopoulos et
al, 2012; Cuadrado, 2016).

72
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Alternative scenario
We suggest that the following actions could strengthen regulation related to conicts
of interest.
• Improving transparency in reporting university-industry interactions. This
could contribute to unveiling institutional and personal conicts of interest of
individual scientists. A potential model to explore is the Sunshine Act, which
was implemented in the US to increase transparency in terms of the doctor-
pharmaceutical industry relationship. For research organisations such as INTA, a
rst step to improve transparency would be to keep updated information on the
Transparency Law website and to issue a conict of interest statement at both an
institutional and an individual level.
• Introducing regulations for researchers participating in industry-funded
foundations. The University of Chile could prohibit membership in industry-funded
foundations and stop accepting scholarships from the food industry. A second-
best option would be to issue guidelines for reporting these conicts of interest in
scientic publications and policy or clinical advisory committees. The creation of
a Conicts of Interest Committee within the University of Chile could represent a
valuable step forward.
• Increasing transparency, monitoring and accountability in decision-making
processes. Requirements for expert participation should be subject to greater
scrutiny. Banning (or imposing restrictions on) people or institutions with ties to
actors with potentially competing interests from participating in policy-making
processes could be seen as an incentive to top researchers to avoid interactions
with the industry. This would also increase the accountability of the process, and
legitimise the decision-making. The processes and guidelines adopted by the
regulatory agencies for pharmacological products such as the Food and Drug
Administration in the US and the European Medicines Agency show how those
changes could be enforced.
• Increasing public and non-industry private funding for research and public health
programmes in food and nutrition. As mentioned above, INTA already has a large
amount of national and international public funding for research. There needs to
be more funding for public health programmes from national and regional levels. In
many cases, only municipalities are eligible for such funding, but INTA already has
extensive experience in collaborating with local governments.

73
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
• Increasing research on conicts of interest and ethical challenges of interactions
between the food industry and public institutions. There is a need to deepen our
knowledge about how these interactions emerge and the motivations for public
institutions to be involved in them. The impact of such interactions on policy-
making is another key area for future research in Chile and elsewhere.
• Increasing the role of civil society. Civil society organisations could be empowered
to become an actor in the accountability of public institutions such as universities.
• The role of the media. The media has a key role in ensuring transparency and
providing information to consumers.
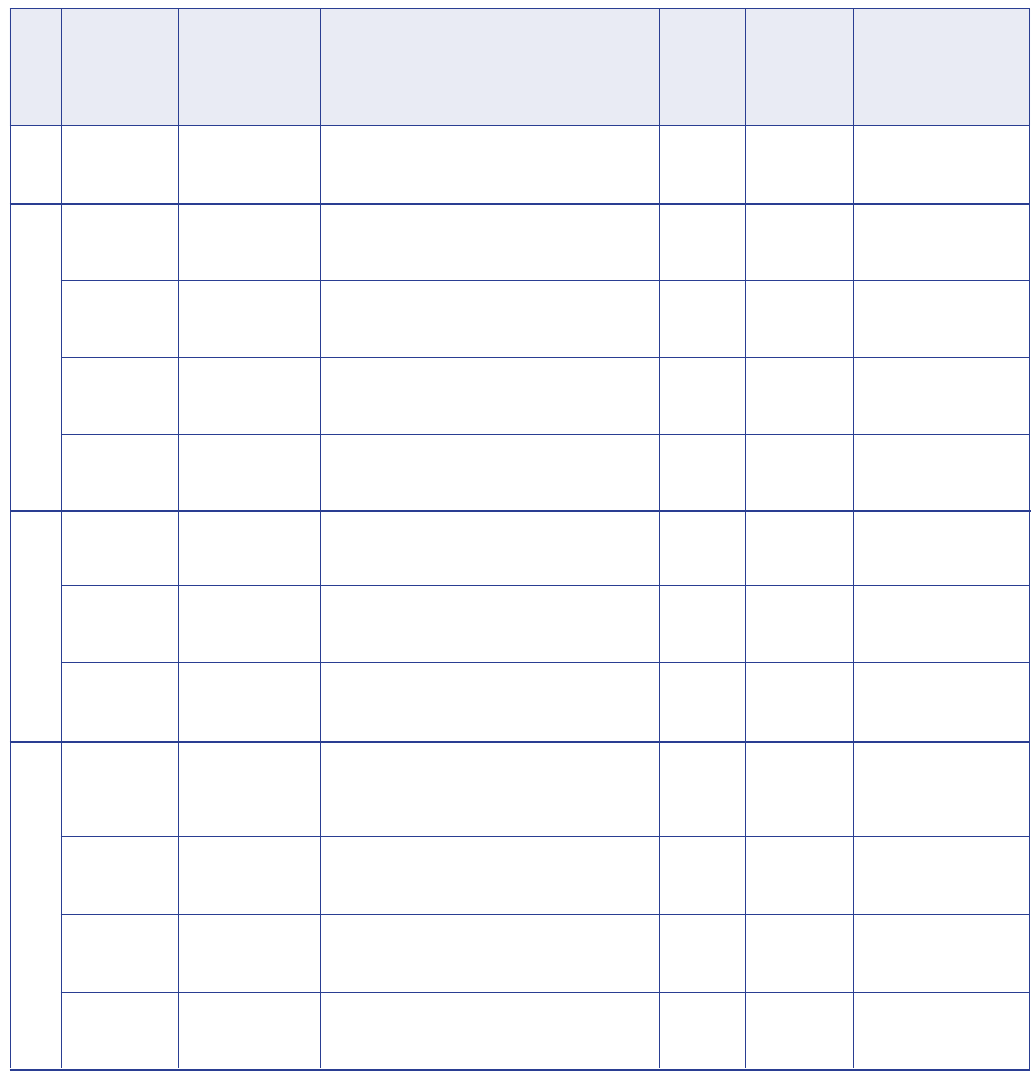
74
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Table 1: Collaboration agreements between INTA and the food and pharmaceutical industry, 2010-2016
Company Type of productsYear
Sopraval
Corpora Tres
Montes
Sociedad
Agrícola Dos
Marías
Corpora Tres
Montes
Cambiaso
Cooperativa
Agrícola y
Pisquera Elqui
CIAL
Danone
Iansagro SA
Surlat
Wrigley
Iansagro SA
2010
2011
2012
2014
Turkey products
Powdered juice and
salty snacks
Vegetables
Powdered juice, salty
snacks and other food
products
Cereals and tea
Pisco (spirit), wine
and juice
Sausages and ham
from pork and turkey
Dairy
Sugar and other food
products
Dairy
Confectionery
Sugar and other food
products
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Food certification of powdered juice Zuko and Zuko
Nutrition. Certificate ‘low in calories’
Certification on microbiological innocuity and
pesticides for ‘Iceberg’ lettuce and ‘Abaco’ carrots
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Food certification of ‘Adelgazul’ brand cereals.
Certificate for low in sodium, high fibre and free of
sugar
Food certification of ‘Atacama juice’ brand juices.
Certification for nutritional content and Omega-3
Food certification for pork, ham, turkey breasts and
turkey ham. Certificate for ‘free of saturated fat, low
cholesterol, free of trans fat’
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Food certification for ‘IANSA’ brand light sugar. INTA
certificates that “Light sugar Iansa allows a reduction
to half a portion, maintaining the equivalent sweetness
as sugar.”
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
330 UF
795 UF
1581.6 UF
165 UF
2112 UF
1035 UF
1627.05 UF
165 UF
2775 UF
165 UF
330 UF
165 UF
for doctors
Certification of a producer
of unhealthy food
Part of a long-term
collaboration with a
producer of unhealthy food
Part of a long-term
collaboration with a
producer of unhealthy food
Certification for the
alcohol industry
Certification of a producer
of unhealthy food
Collaboration with a
producer of unhealthy
food and infant formula
Certification of Chile’s
largest sugar company
Collaboration with a
producer of unhealthy food
Collaboration with a
producer of unhealthy food
Collaboration with Chile’s
largest sugar company
$16,540
$41,795
$83,148
$8,674
$111,033
$55,245
$86,846
$8,807
$125,080
$7,437
$14,874
$7,437
lectures outside
Santiago
Service Amount * CommentaryAmount
in US$
adjusted to
accumulated
inflation **
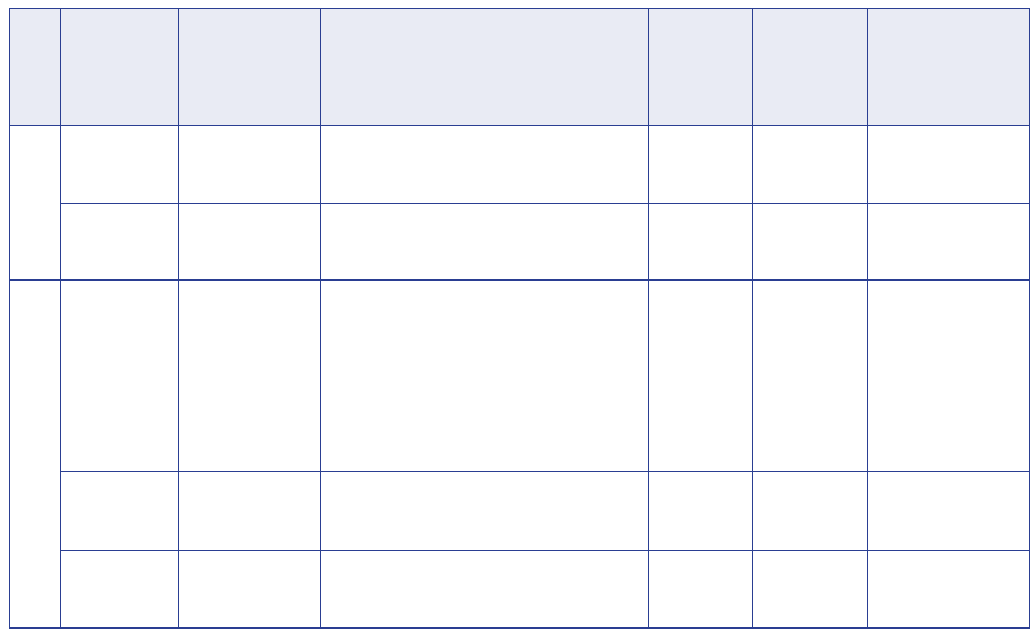
75
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Laboratorio
Pasteur
Surlat
Saval
Ariztía
FRIMA
Year
Pharmaceutical
company
Dairy
Pharmaceutical
company
Poultry
Beef and lamb
processing company
Technical assistance in nutrition, development of new
products, workforce training, literature review, technical
consultations and collaboration in scientific meetings
Food certification for probiotic ‘Surlat kids’. INTA
certificates ‘content of LGG’ (lactobacillus GG)
Educational lectures for doctors and medical
representatives in gastroenterology
Food certification for poultry and turkey brand Ariztía.
INTA certificates products that are ‘low in sodium, free
of gluten and free of soy allergen’
Technical assistance in nutrition, development of new
products, workforce training, literature review and
technical consultations
165 UF
390 UF
Defines fee per
lecture, 16.5
UF for lectures
for doctors
and reps in
Santiago, 24.5
UF for lectures
outside
Santiago
6082 UF
165 UF
Collaboration with a
pharmaceutical company
Certification for a
producer of unhealthy
food
Collaboration with a
pharmaceutical company
Certification of a company
found guilty of collusion
$6,494
$15,350
$634 for lectures
in Santiago;
$941 for lectures
outside Santiago
$233,598
$6,337
Company Type of products
Service Amount * CommentaryAmount
in US$
adjusted to
accumulated
inflation **
2015
2016
* UF is the ‘Unidad de Fomento’, a unit of account issued by the Central Bank of Chile. The unit is
adjusted to inflation and its value changes on a daily basis.
** Value was converted into US$ using the following procedure: UF was converted to Chilean peso
(CLP) using the annual average value for UF according to Internal Tax Administration (Servicios de
Impuestos Internos – SII). CLP was adjusted to inflation using total accumulated inflation according to
SII. Adjusted CLPs were converted into US$ using World Bank Official Exchange Rate for 2010-2015.
Exchange rate for 2016 was the average of observed dollar according to SII (Servicios de Impuestos
Internos, 2016; World Bank, 2016).
Source: Authors’ elaboration based on information received from the University of Chile under the
Transparency Law.
76
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Web edition
Last entry October 16 2016
Issue 14
May to June 2015
Issue 13
January to March 2015
Issue 12
November to December 2014
Issue 11
September to October 2014
Issue 10
July to August 2014
Issue 9
May to June 2014
Issue 8
January to March 2014
Issue 7
December 2013 to January 2014
Issue 6
August to September 2013
Issue 5
April to May 2013
Issue 4
May to June 2012
Issue 3
March to April 2012
Issue 2
December 2011 to January 2012
Issue 1
October to November 2011
Banner
Banner
Banner
2
47
48
2
47
48
2
4
51
52
2
3
51
52
2
5
21
51
52
2
5
20
52
2
5
10
16
22
26
51
52
2
5
10
16
36
51
52
2
4
8
10
51
52
No marketing
10
14
18
14
46
14
24
13
17
13
17
25
Nestlé
Axon-Pharma
Recalcine
Nestlé
Nestlé
Recalcine
Abbott
Aspen Labs
Danone
Nestlé
Iansa
Nestlé
Recalcine
Recalcine
Iansa
Nestlé
Nestlé
Nestlé
Nestlé
Wyeth
Recalcine
Nestlé
Nestlé
Nestlé
Wyeth
Recalcine
Nestlé
Wyeth
Nestlé
Lucchetti
Nestlé
Loncoleche
Nestlé
Recalcine
Loncoleche
Lucchetti
Nestlé
Recalcine
TresMontes
Loncoleche
Wyeth
Nestlé
Wyeth
Loncoleche
Nestlé
Recalcine
Lucchetti
No marketing
Coca-Cola
Nestlé
Loncoleche
Danone
Merck
Nestlé
Nestlé
Loncoleche
Nestlé
Nestlé
Danone
Coca-Cola
Nido
Perenteryl
Biogaia
Chamito
Acticol
Biogaia
Probiotic
Follow-up milk formula
Activia
Chamito
CeroK Sens
Acticol
Biogaia
Biogaia
CeroK Sens
Acticol
Chamito
Premio Henri Nestlé
Chamito
Formula milk
Biogaia
Acticol
Premio Henri Nestlé
Chamito
Follow-up milk formula
Biogaia
Premio Henri Nestlé
Follow-up milk formula
Acticol
Proslow
PIAL
Loncoleche Bio
Chamito
Biogaia
Loncoleche Bio
Proslow
Chamito
Biogaia
Espacio Saludable
Loncoleche Bio
Formula
Public Health Programme in Nutrition
Formula
Loncoleche Bio
Chamito
Biogaia
Proslow
No marketing
Exercise is Medicine
Chamito
Loncoleche Bio
Activia
Forum PKU
Chocapic
Baby food
Loncoleche Bio
Chocapic
Cheerios
Activia
Nestea
Date Page Company Product
Source: Authors’ elaboration based on: Instituto de Nutrición y Tecnología de los Alimentos, 2016a
Table 2: Marketing of the food and pharmaceutical industry in
Nutrition and Life
magazine,
2011-2016
77
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Declarations of interests
Sebastián Peña
Vital Strategies (as part of a project with Bloomberg Philanthropies), National Institute for Health and Welfare, Finnish
Foundation for Alcohol Studies:
• Contract as a consultant with Vital Strategies in support for the Mayors Challenge 2016 from Bloomberg Philanthropies
(2017).
• Consultant for the National Institute for Health and Welfare for the FRESHER Project (funded by the European Union (2017).
• Grant for PhD studies from the Finnish Foundation for Alcohol Studies (2017).
Cecilia Castillo
None declared.
Cristóbal Cuadrado
Ministerio de Salud (Ministry of Health) Chile, Pan-American Health Organization, World Food Program, World Bank, Colegio
Médico de Chile (Chilean Medical Association), NGO Médicos Sin Marca:
• Contracts as consultant for different research-related activities for both national and international governmental institutions.
Honoraria fees dependent on the contract.
• Technical Secretariat at the Department of Public Policy of the Chilean Medical Association. Paid employment.
• Director of the NGO Médicos Sin Marca (Physicians without Brands), promoting a critical culture on the relationships
between industry and physicians in Chile.
Ad honorem
position (no salaries, fees or other financial incentives are received).
María Teresa Valenzuela
None declared.
References
Barquera S, Campos I, Rivera JA (2013). Mexico attempts to tackle obesity: the process, results, push backs and future challenges.
Obesity Reviews,
14 Suppl 2: 69-78.
Bes-Rastrollo M, Schulze MB, Ruiz-Canela M, Martinez-Gonzalez MA (2013). Financial conflicts of interest and reporting bias
regarding the association between sugar-sweetened beverages and weight gain: a systematic review of systematic reviews.
PLoS
Medicine
, 10: e1001578; discussion e1001578
Bolumburu M (2010). Coca-Cola de Chile Presentó su Plataforma de Sustentabilidad: Viviendo Positivamente [Coca-Cola Chile
introduced their Sustainability Platform: Living Positively]. Coca-Cola.
Cruchet S, Lucero Y, Cornejo V (2016). Truths, myths and needs of special diets: attention-deficit / hyperactivity disorder, autism,
non-celiac gluten sensitivity, and vegetarianism.
Annals of Nutrition and Metabolism
, 68, Suppl 1: 43-50.
Cuadrado C (2016). [Public health policies in Chile: seeking to regain trust].
Medwave
, 16 (8): e6532.
Dirección de Asistencia Técnica (2016).
Clientes [Clients]
. Instituto de Nutrición y Tecnología de los Alimentos.
http://www.dinta.cl/clientes/ [Accessed 14 November 2016.]
Dominguez F (2016). Sociedad Chilena de Pediatría decide finalizar su vínculo con Coca Cola. Santiago, Chile:
El Mercurio.
Espacio Saludable (2016).
Espacio Saludable [Healthy Spaces].
http://www.espaciosaludable.cl/ [Accessed 14 November 2016.]
Fisberg M, Maximino P, Kain J, Kovalskys I (2016). Obesogenic environment – intervention opportunities.
Jornal de Pediatria
(Rio J), 92: S30-39.
Fraser B (2013). Latin American countries crack down on junk food.
Lancet,
382: 385-86.
Freedhoff Y, Hebert PC (2011). Partnerships between health organizations and the food industry risk derailing public health
nutrition.
Canadian Medical Association Journal
, 183: 291-92.
Ilsi Sur Andino (2016).
Directorio [Board]
. http://www.ilsisurandino.cl/sitio/ilsi-sur-andino/directorio [Accessed 13 November
2016.]
Institute of Medicine (ed.) (2009).
Conflict of Interest in Medical Research, Education, and Practice.
Washington, DC: The National
Academies Press.
Table 2: Marketing of the food and pharmaceutical industry in
Nutrition and Life
magazine,
2011-2016

78
Public health and the food and drinks industry: The governance and ethics of interactionCASE 6: Chile
Instituto Danone Cono Sur (2016). Asociación Civil Danone para la Nutrición, Salud y Calidad de Vida. http://www.
institutodanoneconosur.org/ [Accessed 13 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2012). INTA inaugura año académico [INTA initiates academic year]. http://
www.uchile.cl/noticias/81394/inta-inaugura-ano-academico [Accessed 13 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2013). Certificación de alimentos para la pequeña y mediana empresa [Food
certification for small and medium enterprises]. https://www.inta.cl/noticia/certificacion-de-alimentos-para-la-pequena-y-
mediana-empresa [Accessed 14 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2014). INTA recibe a estudiantes de posgrado 2014. http://www.inta.uchile.cl/
noticia/inta-recibe-estudiantes-de-posgrado-2014 [Accessed 13 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2015). ILSI premia trabajo de colaboradora del INTA, Mónica Andrews [ILSI
awards work of INTA collaborator, Mónica Andrews]. http://www.inta.uchile.cl/noticia/ilsi-premia-trabajo-de-colaboradora-del-
inta-monica-andrews [Accessed 13 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2016a.)
Nutrición y Vida
[Online]. http://nutricionyvida.cl/ [Accessed 14
November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2016b.)
Programa de Desarrollo del Instituto de Nutrición y Tecnología de
los Alimentos
, Dr Fernando Monckeberg Barros, Universidad de Chile, 2015-2025. http://www.inta.uchile.cl/sites/default/files/
pdi_inta_2016.pdf [Accessed 14 November 2016.]
Instituto de Nutrición y Tecnología de los Alimentos (2016c). Académica del INTA Paulina Correa recibe Beca Malaspina [INTA
researcher Paulina Correa awarded Malaspina Scholarship]. https://www.inta.cl/noticia/academica-del-inta-paulina-correa-
recibe-beca-malaspina [Accessed 13 November 2016.]
International Food Policy Research Institute (IFPRI) (2016).
Global Malnutrition Report 2016. From Promise to Impact: Ending
Malnutrition by 2030
. Washington, DC: International Food Policy Research Institute.
International Nutrition Foundation (2012).
Nevin Scrimshaw International Nutrition Foundation: Annual Report 2012
. http://www.
inffoundation.org/pdf/Annual%20report%202012.pdf [Accessed 14 November 2016.]
International Union of Nutritional Sciences (2009). Memorandum of Understanding (‘MoU’) between the International Union of
Nutritional Sciences and Unilever NV. http://www.iuns.org/wp-content/uploads/2015/07/Memorandum_of_Understanding_
MoU_between_IUNS_and_Unilever_N_V.pdf [Accessed 14 November 2016.]
Kain J, Uauy R, Concha F, et al (2012). School-based obesity prevention interventions for Chilean children during the past decades:
lessons learned.
Advances in Nutrition: An International Review Journal
, 3: 616S-621S.
Katan MB (2007). Does industry sponsorship undermine the integrity of nutrition research?
PLoS Medicine
, 4: e6.
Kearns CE, Schmidt LA, Glantz SA (2016). Sugar industry and coronary heart disease research: a historical analysis of internal
industry documents.
JAMA Internal Medicine
, 176: 1680-85.
La Tercera (2008). Maipú lanza proyecto para disminuir obesidad en escolares de la comuna [Maipú launches project to tackle
obesity in municipal schools].
La Tercera
, 7 May.
Monteiro CA, Cannon G (2012). The impact of transnational ‘big food’ companies on the South: a view from Brazil.
PLoS Med
, 9,
e1001252.
Moodie R, Stuckler D, Monteiro C, et al (2013). Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-
processed food and drink industries.
Lancet
, 381: 670-79.
Nestle M (2013). Conflicts of interest in the regulation of food safety: a threat to scientific integrity.
JAMA Internal Medicine,
173:
2036-38.
Nestle M (2016). Food industry funding of nutrition research: the relevance of history for current debates.
JAMA Internal Medicine
,
176 (11): 1685-86.
Nestlé (2014a). Premio Henri Nestlé cumple 10 años [10 years of the Henri Nestlé Award]. http://www.nestle.cl/media/
pressreleases/premio-henri-nestlé-cumple-10-años
Nestlé (2014b). Reglamento del Décimo Concurso Premio Henri Nestlé a la investigación en nutrición y salud, y tecnología en
alimentos [Rules of the X Henri Nestlé Award for research in nutrition and health and food technology]. http://www.nestle.cl/
media/pressreleases/documents/reglamento_premio_henri_nestle_2014_con%20anexo_v2.pdf [Accessed 13 November 2016.]
Nestlé (2015a). Nestlé en la sociedad: creación de valor compartido y cumplimiento de nuestros compromisos Chile. https://www.
creaciondevalorcompartido.cl/pdf/reporte_de_sustentabilidad_nestle_chile_2015.pdf [Accessed 13 November 2016.]
Nestlé (2015b).
The Nestlé Healthy Kids Global Programme
[Online]. http://www.nestle.com/nutrition-health-wellness/kids-best-
start/children-family/healthy-kids-programme [Accessed 14 November 2016.]

79
Public health and the food and drinks industry: The governance and ethics of interaction CASE 6: Chile
Nestlé (2016).
Nutrición, salud y bienestar: Ayudar a padres, cuidadores y educadores a fomenter hábitos saludables en los niños
[Online]. Nestlé Chile. http://www.creaciondevalorcompartido.cl/nutricion.php [Accessed 29 June 2017]
Pan American Health Organization (2015).
Plan of Action for the Prevention of Obesity in Children and Adolescents
. Washington,
DC: Pan American Health Organization.
Papadopoulos A, Sargeant JM, Majowicz SE, et al (2012). Enhancing public trust in the food safety regulatory system.
Health Policy
,
107: 98-103.
Plataforma de Innovación en Alimentos (2016).
Quienes somos
[Online].http://pialchile.cl/quienes-somos/ [Accessed 14 November
2016.]
PLoS Medicine Editors (2012). PLoS Medicine Series on Big Food: The Food Industry Is Ripe for Scrutiny.
PLoS Medicine
, 9:
e1001246.
Servicios de Impuestos Internos (2017). UF Valores. http://www.sii.cl/pagina/valores/uf/uf2017.htm [Accessed 8 September 2017.]
Uauy R, Aro A, Clarke R, et al (2009). WHO Scientific Update on trans fatty acids: summary and conclusions.
European Journal of
Clinical Nutrition
, 63: S68-S75.
Valenzuela R, Bascunan K, Chamorro R, et al (2015). Modification of docosahexaenoic acid composition of milk from nursing
women who received alpha linolenic acid from chia oil during gestation and nursing.
Nutrients,
7: 6405-24.
Vio del Rio F (2012). Curriculum vitae. http://www.inta.uchile.cl/sites/default/files/cv_fernando_vio.pdf.
World Bank (2017). DataBank: Global Economic Monitor (GEM). http://databank.worldbank.org/data/reports.aspx?source=global-
economic-monitor-(gem) [Accessed 8 September 2017.]
80
Public health and the food and drinks industry: The governance and ethics of interactionCASE 7: Mexico
Authors
Angela Carriedo
London School of
Hygiene and Tropical
Medicine, UK
Carmen Mena
National Institute of
Public Health, Mexico
Claudia Nieto
National Institute of
Public Health, Mexico
Jacqueline Alcalde
National Institute of
Public Health, Mexico
Simón Barquera
National Institute of
Public Health, Mexico
Corresponding
author
Angela Carriedo
Email: angela.
carriedo@lshtm.ac.uk
Summary
The National Strategy to Prevent and Control Overweight, Obesity and Diabetes,
launched in Mexico in 2013, included provision for introducing a mandatory
front-of-package food labelling system. This case study describes how the
labelling strategy was developed, drawing on an analysis of documents, and
interviews with key stakeholders including food industry representatives, policy
ocials, a civil society member, and academic experts on policy, health and
obesity.
The Ministry of Health appointed Cofepris, the food and drug regulatory agency,
to coordinate the design of the new front-of-package labelling. They opened
a public consultation process but, while food industry members recognise
that they actively participated in the process with government ocials, there
was much less involvement of academics and civil society. Furthermore, the
authors of the front-of-package labelling nutrient criteria were three members
of the public entity with no expertise on the topic. This case study reects on
the process and on how transparency and accountability might have been
improved.
The new labelling system is seen as an improvement on self-regulation,
although there is concern that it will be useful mainly for people who already
have some knowledge of nutrition and dietetics, and less useful for the general
public unless it is accompanied by a communication strategy. Civil society
members report that the close relationship between government and the food
industry in the development of the labelling system has resulted in a regulation
that protects the interests of large companies more than the interests of
consumers.
Participation of non-state actors in developing a
food labelling policy in Mexico
7
CASE

81
Public health and the food and drinks industry: The governance and ethics of interaction CASE 7: Mexico
Introduction
In response to rising rates of obesity and diet-related non-communicable diseases
(NCDs) worldwide, several international agencies have provided recommendations
for policy actions to inuence the food environment (Sassi et al, 2009; Mozaarian
et al, 2012). Food labelling is now widely supported internationally as a way to help
consumers make healthier choices when buying packaged foods, and as a tool to
improve food literacy among the population (Cecchini et al, 2010; Hawkes, 2004;
Rayner et al, 2013; Sacks et al, 2013; Swinburn et al, 2013). Several countries in
Latin America are responding to these policy recommendations by changing their
regulations on front-of-package labelling on foods (Campos et al, 2011; Delgado,
2012; Ministerio de Educación, 2013; Pan American Health Organization, 2012;
Vance, 2013).
In an eort to reduce the high burden of obesity in Mexico, the National Strategy to
Prevent and Control Overweight, Obesity and Diabetes was launched in October
2013. It included regulatory changes for a mandatory front-of-package labelling
system. The new regulation, published in 2014, included: a) mandatory front-of-
package nutrition information on saturated fat, ‘other fats’, total sugars, sodium and
energy content per package; and b) a voluntary claim or health logo called a ‘Sello
Nutrimental’, which the food producers could display on products that meet the
nutritional standards for each food group (Secretaría de Salud, 2013).
The political process for this policy development has not been well documented and
the degree of inuence and participation of non-state actors such as civil society,
academics and the food industry remains unclear. Media and press releases made
during the process presented broadly the position of interested groups. This case
study describes the development of the front-of-package labelling strategy, drawing
on an analysis of documents, and interviews with key stakeholders. It explores the
policy design, the participation and inuence of dierent non-state actors, and the
potential conicts of interests surrounding this policy.
We used qualitative research, carrying out semi-structured interviews with 16 actors
including food industry representatives, policy ocials, a civil society member, and
academic experts on policy, health and obesity in 2014. An interview topic guide
was developed to explore the policy design, the context around the process,
and participants’ involvement in, inuence on, and perceptions of the policy. The
interviews were analysed thematically using qualitative methods (Boyatzis, 1998;
Young and Eun-Hee, 2014; Buse et al, 2012; Walt and Gilson, 1994).

82
Public health and the food and drinks industry: The governance and ethics of interactionCASE 7: Mexico
Case
The context for implementing the front-of-package labelling mandatory system
Debates around food labelling have been occurring in Mexico for a long time (Stern
et al, 2011). In 2009 ConMéxico, the largest consortium of food industries in Mexico,
voluntarily introduced front-of-package labelling using the Guideline Daily Amounts
(GDA) system, a strategy which was adopted internationally despite evidence of its
disadvantages (Borgmeier and Westenhoefer, 2009; Campos et al, 2011; Gorton et
al, 2009; Stern et al, 2011).
Academics were advocating for a simple, clear front-of-package labelling system
(Barquera et al, 2013; Carriedo and Barquera, 2013; Cruz-Gongora et al, 2012;
Secretaría de Salud, 2010), and civil society members were demanding clearer,
simpler front-of-package labelling systems, such as a trac-light colouring for
indicating nutrient content (El Poder del Consumidor, 2012). One civil society
interviewee described how, in 2010 and 2013, they presented a public complaint
to the Ministry of Health and had broad media coverage reporting that the front-of-
package labelling system was misleading, and that the reference amount used for
sugar content was too high. It was not until 2012, after the new president had taken
oce, that front-of-package labelling was considered to be included as part of the
regulatory measures to ght obesity (Fundación Mídete, 2015; Secretaría de Salud,
2013).
Front-of-package labelling policy design, and the actors involved
In 2013, the Ministry of Health appointed Cofepris, the food and drug regulatory
agency, to coordinate the front-of-package labelling policy design. They opened a
public consultation process where any person or organisation was entitled to submit
recommendations, resulting in varied and at times contrasting arguments (Sin
Embargo, 2015). There are no ocial records of this participatory approach available
to the general public although, according to a government ocial, they invited
everyone who was known to be working on related topics to participate.
However, a food industry representative mentioned that those attending the public
consultation were mainly seven leaders from the food and beverage industry,
and that there were no representatives from civil society. Moreover, academics
mentioned they had not been invited to participate, and one mentioned that they
had made specic recommendations through the National Academy of Medicine.
Academics proposed a simple labelling system that could inuence buying habits,
based on the World Health Organization nutrient recommendations. The same
interviewee added that front-of-package labelling systems based on GDAs did not
follow or comply with those recommendations.

83
Public health and the food and drinks industry: The governance and ethics of interaction CASE 7: Mexico
In contrast to these accounts, food industry members recognised their active
participation with government ocials. One member of the food industry stated that
the government used the EU Pledge as a reference for the front-of-package labelling
nutrition criteria and adapted it to the Mexican population, although he did recognise
that this labelling system had several shortcomings.
Furthermore, according to an ocial response to a freedom of information request
submitted by civil society members, the authors of the front-of-package labelling
nutrient criteria were three members of the public entity with no expertise on the
topic. The dates and minutes of participants and the evidence used were declared
“non-existent” (Cofepris, 2014). In contrast, an account of a public interview with a
member of Cofepris mentioned that the process went through a public consultation,
and declared that academics and civil society organisations were consulted (Sin
Embargo, 2015).
These inconsistent accounts lead us to reect on the process and how transparency
and accountability might be improved in order to avoid conict of interests among
actors invited to develop the front-of-package labelling system and nutrient criteria.
How can governments protect policy design when opening decision-making to non-
state actors in a controversial scenario?
Perceptions of the front-of-package labelling policy
All of the actors interviewed recognised that the GDA-based front-of-package
labelling system comes from the previous voluntary labelling of the food industry.
While the food industry maintains that they were supporting the Ministry of Health,
some academics and civil society members report that such a close relationship
between government and the food industry resulted in a regulation that protects
the interests of large companies more than the interests of consumers. As one civil
society member mentioned, there was a clear and “serious” conict of interest, as
the food industry is the only non-state actor endorsing this front-of-package labelling
system. He was also of the opinion that dening labelling policy should be the
responsibility of Mexico’s health authorities.
Civil society members perceived that the front-of-package labelling system was
more inclined to protect the industry, that it lacked transparency and that the
process did not include the participation of civil society, and therefore raised these
concerns. The main strength of the regulation was that it was seen to be a step
forward from self-regulation. Interviewees mentioned that the health logo might help
consumers to make healthier choices, which was not the case for the GDA-based
labelling system.

84
Public health and the food and drinks industry: The governance and ethics of interactionCASE 7: Mexico
Regardless of their background, all interviewees considered that the GDA-based
front-of-package labelling mainly addressed people who already have some
knowledge of nutrition and dietetics. It seems less useful for the general public,
unless it is accompanied by a communication strategy.
The final front-of-package labelling strategy policy and reactions
Following the implementation of the labelling strategy, public health experts and
civil society groups publicly declared that the system lacked the rigour needed
to address the Mexican obesity crisis (Servin, 2014; Notimex, 2014). The main
arguments against the policy were:
1 Stricter criteria and simpler formats were needed for the specic Mexican context.
2 There was a lack of information on added sugars or trans fats content – nutrients
known to be related to adverse health outcomes.
3 The labels did not include colour-coding (for high / medium / low levels of
nutrients), even though evidence has shown that this improves consumers’
understanding.
4 The nutrient criteria do not match the cut-o points used in other nutritional
policies (e.g. snack tax and school food guidelines), which may be confusing for
consumers in Mexico (Servin, 2014; Notimex, 2014).
Alternative scenario
An alternative scenario would be to appoint an independent committee of experts
who do not have any conicts of interest to oversee the process, although food
industry leaders might have opposed such a process. It is important to maintain an
inclusive governance process. However, under no circumstances should either the
private sector or civil society decide the nal front-of-package labelling strategy.
If such a scenario were the case, questions about the process would still need
clarication and insight – see the Case questions on the next page.
85
Public health and the food and drinks industry: The governance and ethics of interaction CASE 7: Mexico
Discussion
Case questions
1 What mechanism could ensure that public policy is better designed to improve the health
of the population in addition to declarations of conflicts of interest?
2 How could fair representation of all non-state actors be improved and managed in policy
processes?
3 How could lack of transparency and accountability in policy processes be addressed?
This case study illustrates the role and inuence of non-state actors when designing
policy. Food and beverage industry members have become major players in
designing and setting regulations on food and nutrition, which, as a result, may not
be based on the strongest evidence available. In this case study, it is clear that the
recommendations made by the food industry were considered above those of civil
society or academics. This raises suspicions among other non-state actors and
may impact on the credibility of the policy design and the food industry’s interests in
improving public health.
This case study also highlights the lack of transparency in the consultation process.
Open, public debate is an important part of policy design, given the inherent
competing interests underlying nutrition policy. Furthermore, the context – cultural,
institutional and structural factors – within which a policy is being developed needs
to be carefully considered to ensure health aims are upheld when drafting public
health nutrition regulations.
The primary aim of a front-of-package labelling system is to help consumers to
make healthier choices. As the outcome of the regulation directly aects the primary
interests of the food industry, there is a risk that they could become core actors
in the policy-making process at the expense of consumers. The aim of any food
corporation is to improve revenues by increasing sales and minimising costs – which
are directly impacted by this regulatory change. For example, a requirement to
disclose unhealthy nutrients aects some products that are sold in high volumes.
Products may need to be reformulated either to demonstrate to the consumer that
the product has a reasonable content of unhealthy nutrients, or in order to obtain
the voluntary logo, implying a cost for the producer. There may also be costs for
re-designing packaging. Thus, having a for-prot entity as a key decision-maker on
the best front-of-package labelling available to improve and change consumers’
behaviour towards less packaged food and healthier options is an inherent conict
of interest.
86
Public health and the food and drinks industry: The governance and ethics of interactionCASE 7: Mexico
The primary aim of any public health policy is to improve the health of the population,
using the best available evidence, tools and methods to maximise achievements.
Any secondary aim divergent from the main purpose that might corrupt or endanger
the motivation or decision-making of any of the participants (institutional or personal)
and the achievement of the primary aim is a situation of conict of interest (Marks
and Thompson, 2011; Strech and Knuppel, 2011). Appointing an independent
committee of experts without conicts of interest, to oversee such public policy
processes could help to ensure that public health policy is designed to improve
the health of the population. It could also help to ensure fair representation and
involvement of academics and civil society as core actors in the policy process.
Such policy processes would need to be monitored, and accountability systems
would also need to document clearly the participation of all non-state actors in
both the design and implementation phases (Benner et al, 2004; Kickbusch, 2000;
Kraak et al, 2014; Swinburn et al, 2015). Instruments that have been proposed to
overcome conict of interest in dierent settings include: self-regulation, disclosures,
report of potential bias and how it is managed, codes of ethics during discussions,
and accountability measures such as assessment, communication, enforcement,
and improvement (remedial actions) (Rodwin, 2015; Swinburn et al, 2015).
Declarations of interests
Angela Carriedo
None declared.
Carmen Mena
None declared.
Claudia Nieto
None declared.
Jacqueline Alcalde
None declared.
Simón Barquera
Processed food and beverage industry:
I was part of the Hydration for Health Initiative expert advisory committee to promote
hydration with water. They covered travel costs to their international experts meeting. I did not receive remuneration.
Bonafont sponsored a research project at my research centre to promote water consumption in the population to reduce
metabolic syndrome. I collaborated in this project.
Pharmaceutical:
Novonordisk, Sanofi-Aventis, Silanes and Ifaceltics sponsored research projects at my centre (descriptive
epidemiological studies from surveys). These studies did not test any drug or specific treatment. The funding was unrestricted
and the funders did not discuss research results or reports.
Weight loss industry:
I have participated in advisory board meetings for Medifast and Herbalife (companies with meal
replacement programmes to treat obesity). In these meetings I presented obesity trends in Mexico and national efforts to prevent
and control the epidemic.

87
Public health and the food and drinks industry: The governance and ethics of interaction CASE 7: Mexico
References
Barquera S, Campos I, Rivera J (2013). Mexico attempts to tackle obesity: the process, results, push backs and future challenges.
Obesity
Reviews
, 14 (S2): 69-78.
Benner T, Reinicke WH, Witte JM (2004). Multisectoral networks in global governance: towards a pluralistic system of accountability.
Government and Opposition
, 39 (2): 191-210.
Borgmeier I, Westenhoefer J (2009). Impact of different food label formats on healthiness evaluation and food choice of consumers: a
randomized-controlled study.
BMC Public Health
, 9: 184.
Boyatzis RE (1998).
Transforming Qualitative Information: Thematic Analysis and Code Development
. Sage Publishing.
Buse K, Mays N, Walt G (2012).
Making Health Policy
. London: McGraw-Hill Education.
Campos S, Doxey J, Hammond D (2011). Nutrition labels on pre-packaged foods: a systematic review.
Public Health Nutrition
, 14 (8):
1496-1506.
Carriedo A, Barquera S (2013).
Sistema Voluntario de Etiquetado Frontal de Alimentos en México: Antecedentes, Bases Técnicas y
Propuesta de Implementación
. Mexico: Centro de Investigación en Nutrición y Salud, Instituto Nacional de Salud Pública.
Cecchini M, Sassi F, Lauer JA, et al (2010). Tackling of unhealthy diets, physical inactivity, and obesity: health effects and cost-
effectiveness.
The Lancet
, 376 (9754): 1775-84.
Cofepris (2014).
Oficio No. CGJC/OR/355/2014
, Mexico.
Cruz-Gongora V, Villalpando S, Rodriguez-Oliveros G, et al (2012). Use and understanding of the nutrition information panel of pre-
packaged foods in a sample of Mexican consumers.
Salud Pública de México
, 54 (2): 158-66.
Delgado J (2012).
Perú: Ley contra Obesidad en Niños en Perú y Papel del Parlatino en la Estrategia: Ley Marco para América Latina sobre
la Regulación de la Publicidad de Alimentos
. Paper presented at Legislación, normas y políticas públicas para detener la obesidad y
promover alimentación saludable entre los niños de Latinoamérica: avances, obstáculos y posiblidades. Mexico DF.
El Poder del Consumidor (2012). El fin del Acuerdo Nacional por la Salud Alimentaria (ANSA) y la Necesidad de una Ley y Política Integral
de Combate a la Obesidad. http://www.elpoderdelconsumidor.org/wp-content/uploads/Documento-ANSA.pdf [Accessed 12 June 2012.]
Fundación Mídete (2015). La Necesidad de una Ley General contra la Obesidad.
http://bioeticacotidiana.blogspot.co.uk/2015/03/la-necesidad-de-una-ley-general-contra.html
Gorton D, Mhurchu CN, Chen MH, Dixon R (2009). Nutrition labels: a survey of use, understanding and preferences among ethnically
diverse shoppers in New Zealand.
Public Health Nutrition
, 12 (9): 1359-65.
Hawkes C (2004).
Nutrition Labels and Health Claims: The Global Regulatory Environment.
World Health Organization.
Kickbusch I (2000). The development of international health policies – accountability intact?
Social Science and Medicine
, 51 (6): 979-89.
Kraak VI, Swinburn B, Lawrence M, Harrison P (2014). A Q methodology study of stakeholders’ views about accountability for promoting
healthy food environments in England through the Responsibility Deal Food Network.
Food Policy
, 49, Part 1: 207-18. doi:
http://dx.doi.org/10.1016/j.foodpol.2014.07.006
Marks JH, Thompson DB (2011). Shifting the focus: conflict of interest and the food industry.
American Journal of Bioethics
, 11 (1), 44-46.
doi: 10.1080/15265161.2011.534953
Ministerio de Educación (2013). Ley Nº 30021: Ley de Promoción de la Alimentación Saludable para Niños, Niñas y Adolescentes.
El
Peruano
(494937-9).
Mozaffarian D, Afshin A, Benowitz NL, et al (2012). Population approaches to improve diet, physical activity, and smoking habits: a
scientific statement from the American Heart Association.
Circulation
, 126 (12): 1514-63.
Notimex (2014). Propone el INSP etiquetado con un sello binario para alimentos industrializados.
http://www.jornada.unam.mx/2014/02/24/sociedad/042n1soc [Accessed 13 October 2014.]
Pan American Health Organization (2012). Se aprueba ley de composición nutricional de los alimetos y su publicidad en Chile.
http://www.paho.org/hq/index.php?option=com_content&view=article&id=7057%3A2012-se-aprueba-ley-composicion-nutricional-
alimentos-publicidad-chile&catid=1443%3Aweb-bulletins&Itemid=135&lang=es [Accessed October 2016.]
Rayner M, Wood A, Lawrence M, et al (2013). Monitoring the health-related labelling of foods and non-alcoholic beverages in retail
settings.
Obesity Reviews
, 14 (S1): 70-81.
Rodwin MA (2015). Do we need stronger sanctions to ensure legal compliance by pharmaceutical firms?
Food and Drug Law Journal
, 70
(3): 15-31.
Sacks G, Swinburn B, Kraak V, et al (2013). A proposed approach to monitor private-sector policies and practices related to food
environments, obesity and non-communicable disease prevention.
Obesity Reviews
, 14 (S1): 38-48.

88
Public health and the food and drinks industry: The governance and ethics of interactionCASE 7: Mexico
Sassi F, Cecchini M, Lauer J, Chisholm D (2009).
Improving lifestyles, tackling obesity: the health and economic impact of prevention
strategies. OECD Health Working Papers
, 48 (106).
Secretaría de Salud (2010).
Bases Técnicas del Acuerdo Nacional para la Salud Alimentaria: Estrategia Contra el Sobrepeso y la Obesidad.
Mexico, DF.
Secretaría de Salud (2013).
Estrategia Nacional para la Prevención y el Control del Sobrepeso, la Obesidad y la Diabetes.
Mexico: Secretaría de Salud.
Servin R (2014). Señalan que etiquetado en alimentos es engañoso y pone en riesgo la salud. http://www.elfinanciero.com.mx/sociedad/
etiquetado-enganoso-en-alimentos-y-bebidas-pone-en-riesgo-la-salud.html [Accessed 14 October 2016.]
Sin Embargo (2015). Entrevista: Comisionado de Cofepris rechaza estar al servicio de la industria, como dicen ONGs.
http://www.sinembargo.mx/09-03-2015/1273606
Stern D, Barquera S, Tolentino L (2011).
Revisión del Etiquetado Frontal: Análisis de las Guias Diarias de Alimentación (GDA) y su
Comprensión por Estudiantes de Nutrición en México.
Mexico: Instituto Nacional de Salud Pública.
Strech D, Knuppel H (2011). How to evaluate conflict of interest policies.
American Journal of Bioethics
, 11 (1): 37-39. doi:
10.1080/15265161.2011.534956
Swinburn B, Sacks G, Vandevijvere S, et al (2013). INFORMAS (International Network for Food and Obesity/non-communicable diseases
Research, Monitoring and Action Support): overview and key principles.
Obesity Reviews
, 14 (S1): 1-12.
Swinburn B, Kraak V, Rutter H, et al (2015). Strengthening of accountability systems to create healthy food environments and reduce global
obesity.
The Lancet
, 385 (9986): 2534-45. doi: http://dx.doi.org/10.1016/S0140-6736(14)61747-5
Vance C (2013). Reglamento Sanitario de Etiquetado de Alimentos Procesados para el Consumo Humano.
http://www.controlsanitario.gob.ec/wp-content/uploads/downloads/2014/08/REGLAMENTO-SANITARIO-DE-ETIQUETADO-DE-
ALIMENTOS-PROCESADOS-PARA-EL-CONSUMO-HUMANO-junio-2014.pdf [Accessed 14 October 2016.]
Walt G, Gilson L (1994). Reforming the health sector in developing countries: the central role of policy analysis.
Health Policy and
Planning
, 9 (4); 353-70.
Young CJ, Eun-Hee L (2014). Reducing confusion about grounded theory and qualitative content analysis: similarities and differences.
The
Qualitative Report
, 19 (32): 1-20. doi: http://nsuworks.nova.edu/tqr/vol19/iss32/2
89
Public health and the food and drinks industry: The governance and ethics of interaction CASE 8: Guatemala
Summary
Since 2011, in all Central American countries including Guatemala, all packaged
foods with health claims must include information about the type and quantity of
each nutrient in a ‘nutrition facts label’, but consumers nd these confusing and
dicult to understand.
We conducted a research project, in Guatemala City, to develop and test three
front-of-package labels, aimed at informing consumers about the health risks
of sugar-sweetened beverages (SSBs). The rst label showed the amount of
sugar in each drink and the adult Guideline Daily Amount (GDA) for sugar. The
second was a ‘trac-light’ label, which gave the percentage of the adult GDA in
the drink within a red trac light. The third label stated “The consumption of this
beverage contributes to obesity and diabetes.”
A private marketing company with more than 18 years’ experience in building
brands for food and beverage companies in Guatemala was hired by our
research team to design the labels. International experts in cigarette and food
labelling and warning label implementation were consulted during the label
design process.
The rst label – which gave sugar content and GDA – was found to be the most
confusing and least appealing. Participants said the second label – of the trac
light and GDA – was eye-catching but confusing. The third option – the warning
label – caught their attention the most and participants found it informative
about the consequences of sugar consumption.
The partnership with a design company that had worked for the beverage
industry poses certain ethical and political questions, as we were hiring them to
design labels that would potentially be used to undermine the interests of food
and beverage corporations by guiding consumers into moderating consumption
or making alternative choices. It highlights the question of whether and how
public health researchers and practitioners navigate existing relationships
between marketing companies, research units, and industry actors.
Designing a front-of-package labelling system
to encourage healthier beverage choices in
Guatemala
8
CASE
Authors
Violeta Chacon
Department of Research,
Cardiovascular Surgery
Unit of Guatemala
Peter Benson
Department of
Anthropology,
Washington University in
St Louis, USA
Joaquin Barnoya
Department of Research,
Cardiovascular Surgery
Unit of Guatemala
Division of Public Health
Sciences, Department
of Surgery, Washington
University in St Louis,
USA
Corresponding author
Violeta Chacon
Email: violetachacon@
gmail.com

90
Public health and the food and drinks industry: The governance and ethics of interactionCASE 8: Guatemala
Introduction
Guatemala, a lower-middle-income country, is currently contending with the double
burden of malnutrition (Ramirez-Zea et al, 2014). The level of childhood stunting
in Guatemala is one of the highest worldwide (49%), and overweight and obesity
combined is also high, especially among women (49.4%) (Ministerio de Salud
Pública y Asistencia Social et al, 2011). Among other factors, the consumption of
sugar-sweetened beverages (SSBs) is a key contributor to the obesity epidemic in
low-/middle-income countries such as Guatemala.
The level of consumption of SSBs in Guatemala is one of the highest in Latin
America (women drink 2.69 servings per day, and men 2.90 servings) (Singh et al,
2015) and it is linked to large-scale dynamics of global capitalism. The increased
market penetration of Coca-Cola and other soft drinks in urban and rural Guatemala
has dramatically altered the food environment over time and resulted in the
ubiquitous presence of SSBs (Nagata et al, 2011). In addition, energy-dense foods
and beverages are readily available and heavily marketed, with marketing eorts that
especially target school-aged children (Chacon et al, 2013). In the absence of public
policies that constrain the capacity of multi-national corporations to manufacture
foods and beverages cheaply and penetrate markets, one alternative is to help
consumers make more informed choices by providing labels that give clear and
accurate nutrition information.
In 2011, all Central American countries, including Guatemala, adopted the Central
American Technical Regulation, which provides regulatory provisions for food
packaging (Consejo de Ministros de Integración Económica, 2011). According to the
Regulation, all packaged foods with health claims must include information about
the type and quantity of each nutrient in a ‘nutrition facts label’. This label should
be presented as text within an outlined box on the packaging. However, previous
research has found that most consumers have diculty understanding and using
nutrition facts labels because of the confusing nature of the information (Mazariegos
and Barnoya, 2016). To date, there has been no evaluation of the nutrition facts
label as a tool for guiding and promoting healthy food choices. It is therefore crucial
to design and test alternative labelling systems, such as front-of-package labels
(Hawley et al, 2013; Roberto et al, 2016). This alternative form of labelling has the
potential to provide consumers with nutrition information that is accurate and easier
to understand, and that helps them to make informed choices.
We conducted a research project to develop and test three front-of-package labels,
specially designed for the Guatemalan market and aimed at informing consumers
about the health risks of SSBs. The research setting was Guatemala City, the

91
Public health and the food and drinks industry: The governance and ethics of interaction CASE 8: Guatemala
country’s capital city, a large urban centre. Three labels were tested. The rst label,
a black and white box, displayed the amount of sugar contained in each drink,
the adult Guideline Daily Amount (GDA) for sugar, and the percentage of the GDA
represented by the amount of sugar in the beverage. (The adult GDA for sugar is the
maximum amount of sugar recommended per day for an adult.) The second label
was a ‘trac-light’ label, which indicated that the product contained a high amount
of sugar by showing the percentage of the adult GDA in the drink, within a red trac
light. The third label, which included the text “The consumption of this beverage
contributes to obesity and diabetes”, gave an explicit warning to consumers about
the health hazards of SSBs. This project was conducted by researchers at a public
cardiac surgery centre in Guatemala City and aimed to produce and compare
consumer-friendly labelling systems to identify the most eective type of label that
the Guatemalan government could use to better inform consumers of the nutritional
value and health risks associated with SSBs.
Case
Before designing the consumer-tailored labels, we rst conducted a systematic
literature review to gather information regarding the design and impact of dierent
front-of-package and warning label systems. We also identied the front-of-package
label systems that have already been implemented in dierent countries across Latin
America.
A private marketing agency with more than 18 years’ experience in building brands
and creating logos for food and beverage companies in Guatemala was hired to
design the labels. The hiring process did not involve a request for proposals and
this particular company was the only design company considered. The decision to
hire this company reected the fact that we had previously worked with them on the
design and development of snack food packages to test how licensed characters
(e.g. mascots) inuence children’s taste and snack preferences. The company’s
experience with the food industry and previous collaboration with our team were
the main reasons for hiring it to design the labels and organise focus groups for our
research.
International experts – including two very experienced researchers in cigarette and
food labelling, and one of the principal investigators on the study that supported
warning label implementation in Chile – were consulted during the label design
process. These experts were invited to be consultants during the preparation of
the research proposal, on the basis of their expertise. They were asked to provide
feedback via e-mail or conference calls on the study design and implementation.
The preliminary label designs were sent to them by e-mail, and the experts provided

92
Public health and the food and drinks industry: The governance and ethics of interaction
feedback on the design elements (e.g. using only the colour red for the trac-
light label), position, and wording. Their feedback was well received by the design
company and was incorporated into the design of the labels for our trial. The
company also provided important feedback from its vast experience of designing
labels for the food industry. It recommended the colour combinations with the
highest visibility for the front-of-package labels, as well as typography fonts and
shapes (e.g. a triangle with an exclamation mark to symbolise danger). One of the
challenges that came up during the design process involved the size of the labels.
Even though the experts recommended that the size should be 25%, there is no
evidence to prove that this size yields the best visibility. In addition, our partner
company was not able to comply entirely with this recommendation because the
packaging of the beverages we were testing came in various dierent shapes,
which made it dicult to apply the same label to all beverages. For example, the
text warning label was a rectangular shape, so it was easy to apply it to beverages
with similar shaped packages. However, when it was applied to square-shaped
packages, it was dicult to keep the consistency of the size and shape of the
label. The design company therefore recommended that the shape of the beverage
packages should determine the label size.
Once the design company had produced the labels, it conducted six focus groups
– two with adolescents, two with male caregivers, and two with female caregivers
– to evaluate consumers’ understanding of the labels and their design preferences.
Since the company was going to conduct the focus groups and interpret the data,
our team developed a focus group guide with help from our international experts, to
make sure that the underlying research objectives were met. The design company
also contributed to the development of the focus group guide by adding questions
to stimulate spontaneous reactions and activities to compare participant perceptions
of the dierent labels. The company was able to recruit the focus group participants
in two days due to its large network and experience in the eld. They also provided
an adequate location and a trained focus group moderator. One of the members of
our research team audited the focus groups to ensure that the marketing company
adhered to the focus group guide.
In terms of the participants’ understanding of the labels and the interpretation by
the design company, the rst label – which gave sugar content and GDA – was the
most confusing and least appealing. This label appeared familiar to participants
because some beverage companies had already voluntarily introduced it. The
second option – of the trac light and GDA – attracted the participants’ attention,
but they thought it was confusing. The third option – the warning label – caught their
attention the most. They said the message made them think twice about drinking
CASE 8: Guatemala

93
Public health and the food and drinks industry: The governance and ethics of interaction CASE 8: Guatemala
the beverage. Some participants thought that the warning label gave them a clear
prohibitive message and they appreciated that it provides more details about the
consequences of sugar consumption.
The design company concluded that the warning label had the most potential to
inform consumers. In addition, it recommended avoiding the use of the colour red,
because of the extensive amount of red already used on SSB labels (e.g. Coca-
Cola). They recommended that the warning label be placed as a header around
the top of the beverage container, and not as a rectangle on one side, so that the
label is visible from all angles of the beverage. Finally, the company recommended a
marketing campaign to create consumer awareness of the front-of-package labels in
Guatemala, similar to when beverage companies launch new products.
Alternative scenario
If we had not hired the particular marketing company that we did, our team would
have conducted the label design and focus groups on our own. The label design
would have been based solely on the opinions of our collaborating experts and a
literature review, and would therefore not have included the input of the company.
Important design issues brought up by the design company would have been left
out, and it is crucial to acknowledge that the partner company has vast experience
in designing and implementing product packaging and labels in the Guatemalan
context.
However, we acknowledge that this partnership poses certain ethical and political
questions that are germane to the research and the overall aims of public health.
The partner company has worked for the beverage industry, and in this instance
we hired them to design labels that would potentially be used to undermine the
interests of food and beverage companies by guiding consumers into moderating
consumption or making alternative choices. Our partnership with the company
thus presents a challenging case study related to the question of whether and how
public health researchers and practitioners navigate existing relationships between
marketing companies, research units, and industry actors.
94
Public health and the food and drinks industry: The governance and ethics of interaction
Discussion
Case question
What measures should public health researchers take in order to avoid conflicts of interest
when working with private marketing companies?
The local marketing company with which we partnered was able to design a
consumer-friendly front-of-package label and obtain consumer perceptions of
dierent types of labels. It was also able to help us interpret the results from the
industry’s standpoint. There were some disagreements between the marketing
company and our research team, and our case study raises an interesting question
about the possibility that public health researchers may disagree with a private
marketing company over issues such as label design, questions to be asked at
focus groups, or data analysis and interpretation. There is also the question of how
the marketing company’s economic and political interests might inuence the results
of the research or its interpretations.
The potential ethical challenge that emerged from our interaction with the marketing
company centered on its previous work for food and beverage companies that
would be likely to oppose the implementation of a front-of-package label in
Guatemala. Given that there is an inherent conict of interest between the goals
of this kind of public health research and policy implementation and the food
companies that have previous relationships with marketing and design companies,
we made sure that we clearly stated the project objectives when we undertook our
collaboration in order to align our team’s and the marketing company’s goals from
the start. This level of transparency was a means of overcoming the potential conict
of interest and ensuring that the work of the marketing company aligned with the
public health research and practice goals. In addition, to ensure this alignment, one
of the members of our team worked closely with the marketing company during the
entire process of research, analysis and label design.
Governance of interactions between researchers and private marketing companies
could be strengthened not only by the alignment of academic and practical goals,
but also by assessing and evaluating the roles, strengths and limitations of each
of the actors. Researchers are important actors in generating evidence to support
policies that benet public health. However, in lower-middle-income countries
like Guatemala, resources for public health research are limited and so there is a
situation in which researchers and practitioners have an economic and political
incentive to partner with private marketing and research assessment companies that
can contribute expertise and resources in a number of areas, from social marketing
CASE 8: Guatemala

95
Public health and the food and drinks industry: The governance and ethics of interaction CASE 8: Guatemala
campaigns to market research for product development and tools to promote
health or label foods. Currently, there are no governance guidelines for interactions
between researchers and marketing companies. If such guidelines – for example, a
system of best practice recommendations or regulations – were to be created, what
should they include? Who should be involved in creating these guidelines? We are
not giving answers to these questions at this point. The purpose of raising these
questions is simply to reect on the relationships and interests that we encountered
in our eorts to improve nutrition labels in Guatemala, and to suggest that the need
for public-private partnerships in resource-limited settings demands heightened
levels of governance, regulation, oversight and research.
Acknowledgments
This work was carried out with the aid of a grant from the International Development Research Centre, Ottawa, Canada. Joaquin
Barnoya receives additional support from an unrestricted grant from The Foundation for Barnes-Jewish Hospital.
Declarations of interests
Violeta Chacon
None declared.
Peter Benson
None declared.
Joaquin Barnoya
None declared.
References
Chacon V, Letona P, Barnoya J (2013). Child-oriented marketing techniques in snack food packages in Guatemala.
BMC Public
Health
, 13: 967. doi: 10.1186/1471-2458-13-967
Consejo de Ministros de Integración Económica (2011).
Etiquetado Nutricional de Productos Alimenticios Preenvasados para
Consumo Humano para la Población a Partir de 3 Años de Edad
. Guatemala.
Hawley KL, Roberto CA, Bragg MA, et al (2013). The science on front-of-package food labels.
Public Health Nutrition
, 16 (3): 430-
39. doi: 10.1017/S1368980012000754
Mazariegos M, Barnoya J (2016). Nutrition label use in a Latin American middle-income country: Guatemala.
Food and Nutrition
Bulletin
, 38 (1): 128-32.
Ministerio de Salud Pública y Asistencia Social, Instituto Nacional de Estadística, Universidad del Valle de Guatemala, Agencia de
los Estados Unidos para el Desarrollo Internacional, et al (2011).
V Encuesta Nacional de Salud Materno Infantil 2008-2009
.
Guatemala.
Nagata JM, Barg FK,
Valeggia CR, Bream KD (2011)
.
Coca-colonization and hybridization of diets among the Tz’utujil Maya.
Ecology of Food and Nutrition
, 50 (4): 297-318. doi: 10.1080/03670244.2011.568911
Ramirez-Zea M, Kroker-Lobos MF, Close-Fernandez R, Kanter R (2014). The double burden of malnutrition in indigenous and non-
indigenous Guatemalan populations.
American Journal of Clinical Nutrition
, 100 (6): 1644S-51S. doi: 10.3945/ajcn.114.083857
Roberto CA, Wong D, Musicus A, Hammond D (2016). The influence of sugar-sweetened beverage health warning labels on parents’
choices.
Pediatrics
, 137 (2): e20153185. doi: 10.1542/peds.2015-3185
Singh GM, Micha R, Khatibzadeh S, et al, Global Burden of Diseases Nutrition and Chronic Diseases Expert Group (2015). Global,
regional, and national consumption of sugar-sweetened beverages, fruit juices, and milk: a systematic assessment of beverage
intake in 187 countries.
PLOS One,
10 (8): e0124845. doi: 10.1371/journal.pone.0124845
96
Public health and the food and drinks industry: The governance and ethics of interactionCASE 9: Spain
Authors
Ildefonso Hernández-
Aguado
Department of
Public Health, Miguel
Hernández University,
Alicante, Spain
CIBER de
Epidemiología
y Salud Pública
(CIBERESP), Alicante,
Spain
Joan R Villalbí
Agència de
Salut Pública de
Barcelona, Barcelona,
Spain
CIBER de
Epidemiología
y Salud Pública
(CIBERESP), Alicante,
Spain
Institut
d’Investigacions
Biomèdiques Sant
Pau, Barcelona,
Spain
Departament
de Ciències
Experimentals i de
la Salut, Universitat
Pompeu Fabra,
Barcelona, Spain
Corresponding
author
Ildefonso Hernández-
Aguado
Email: ihernandez@
umh.es
Summary
The alcohol industry has been successful in preventing attempts at improving
regulatory policies relating to alcohol in Spain. The main players opposed to
alcohol regulation are three trade organisations: the Spanish Federation of
Spirits Producers, the Association of Beer Manufacturers, and the Federation
of Wine Producers. Although these organisations do not always concur in
their interests, all three avoid regulations by promoting self-regulation and
agreements with the government.
There is a normalised environment of continuous exposure to a variety of
alcohol products and marketing in Spain. Through successful public relations
campaigns, the alcohol industry has shaped a public climate favourable to
agreements. In this context, the alcohol industry proposed collaborations with
the government to prevent under-age alcohol consumption. The challenge
for public health decision-makers lies in the risks posed by engaging in such
partnerships of high public and political acceptance that may jeopardise
eective regulation. This case study looks at public-private interaction with the
alcohol industry in Spain.
Public-private interaction with the alcohol
industry and failures in the regulation of alcohol
in Spain
9
CASE

97
Public health and the food and drinks industry: The governance and ethics of interaction CASE 9: Spain
Introduction
The alcohol industry has been successful in preventing three attempts at improving
regulatory policies related to alcohol in Spain. In 2002, in reaction to the increasing
perception of heavy drinking in the streets by adolescents and young adults, the
conservative government promoted a bill to address some aspects of availability and
advertising of alcoholic drinks. This was met with a virulent reaction of interested
agents, the socialist party, and youth organisations, and was eventually shelved
after a cabinet reshue (Rodriguez Martos, 2007). In 2008, a similar proposal by the
socialist government to reduce alcohol availability and advertising was blocked by
interested agents and the conservative party, who staged a erce reaction (Villalbí et
al, 2008). The last attempt at regulation, by another conservative government in 2012,
focused nominally on minors and, as well as banning sales to under-18s (already
banned in 16 of the 17 regional administrations), it also included restrictions on
sponsorship and advertising and some limitations on availability. The bill met with opposition
from interested actors, and was eventually shelved after three years of consultations.
The main actors opposed to alcohol regulation are the three trade organisations:
the Spanish Federation of Spirits Producers, the Association of Beer Manufacturers,
and the Federation of Wine Producers. Although these three organisations do
not always concur in their interests, they all avoid regulations by promoting self-
regulation and agreements with the government. The Federation of Food and
Drink Industries, to which all three belong, is the umbrella organisation for lobbying
activities. The alcohol producers do not operate in isolation: their high investment in
publicity, sports and music sponsorship has a signicant impact on how the public
perceives their role. Spirit producers have been active in showing their commitment
to the prevention of drinking in vulnerable populations by developing campaigns to
discourage consumption among young people and pregnant women. Many of these
activities are channelled through public relations organisations that have engaged
high-prole academics on their advisory or scientic committees and established
links with medical associations. On the public health side, the actors committed
to the prevention of alcohol abuse have not yet reached a level of organisation
comparable to that of the anti-tobacco movement that proved so eective (Córdoba
et al, 2006; Hernández-Aguado, 2013). The population still suers from a high
burden of morbidity attributable to alcohol consumption (Sarasa-Renedo et al,
2014).
The successful public relations campaigns of the alcohol industry have shaped
a public climate favourable to agreements between the sector and the public
administrations. Furthermore, Spanish cities provide a normalised environment of
continuous exposure to a wide variety of alcohol products and marketing (Sureda et al,

98
Public health and the food and drinks industry: The governance and ethics of interactionCASE 9: Spain
2017). In that context, the alcohol industry proposed the establishment of
collaborations with the government in order to prevent under-age alcohol consumption.
The challenge for public health decision-makers lies in the risks posed by engaging
in partnerships of high public and political acceptance that could jeopardise eective
regulation. While some actions of the alcohol industry are obvious attempts at
inuencing policy and can be avoided through appropriate public health ethical
codes or guidelines, others are more dicult to prevent as they appear to occur in
the natural course of events. Below, we present a case study of public health policy
related to the alcohol industry and its activities.
Case
Since the 1990s, the alcohol industry in Spain has developed a systematic strategy
to propose to the government voluntary agreements aimed at preventing under-
age consumption of alcohol and promoting self-regulation in advertising. In 2010,
they persuaded top ocials at the Ministry of Health to insist that the Public Health
Directorate should engage in a partnership with alcohol producers in order to
achieve zero alcohol consumption among adolescents. The Chief Public Health
Ocer had to decide whether to endorse the proposal drafted by the industry – by
convincing the Minister to sign a code of self-regulation regarding alcohol advertising
– or to resist the pressure.
The Ministry of Health was the key player as its participation would facilitate the
recruitment of many other actors such as members of parliament, non-governmental
organisations, medical associations, trade unions, consumer associations,
hospitality associations, and the mass media federation. The endorsement could
be highly benecial for the government, presenting a wide social agreement across
many sectors with a praiseworthy objective. Most other actors might have felt that
it was a consensual action, perceived as good by the public. Of course, it was also
to the advantage of the alcohol industry, as it appeared to support a good cause.
The decision-maker would nd it dicult to identify downsides of the programme
as there are no risks to personal freedom or justice. The proposed partnership
ostensibly sought to protect the vulnerable – children and adolescents – as
recommended in public health ethical frameworks (Nueld Council on Bioethics,
2007). Furthermore, it seemed to t the recommendation for the industry: to
recognise more fully the vulnerability of children and young people, and take clearer
responsibility for preventing harm to health. As the government would not incur any
direct costs, the issue of the eectiveness of the partnership in achieving its stated
goals may have been perceived as secondary in the decision-making process.
Public health ethical codes include eectiveness of policies and programmes as a

99
Public health and the food and drinks industry: The governance and ethics of interaction CASE 9: Spain
prerequisite. However, other relevant factors to be considered in this particular case
are the risks that the decision could pose to the future role of government in stricter
alcohol regulation. It is also important to consider the potential for the partnership
to contribute to a positive social image of the alcohol industry, as well as possible
future conicts of interest, particularly taking into consideration the frequency of
various types of conict, including ‘revolving doors’ (Villoria and Revuelta, 2014).
Despite initial reticence in the Public Health Directorate of the Ministry of Health, the
industry took advantage of a government reshue and was successful in engaging
the new Minister of Health in signing the code of self-regulation in 2011. After the
2012 elections, which led to a major change in government, the Ministry of Health
established a similar agreement with the Federation of Spirits Producers. The media
gave a positive welcome to both deals and highlighted the degree of consensus
among players. However, infringements of the code occurred from the very outset
(for example, images of famous footballers appeared on beer cans, in violation of
the rst rule of the code) and the Ministry failed to react. Unlike actual regulations,
self-regulatory industrial codes mean that the administration is essentially excluded
from the laissez faire loop and may not even be aware of infringements. Moreover,
when signing the second agreement mentioned above, the Ministry of Economy
made provision for the deregulation of many aspects of trade, including a measure
that abolished a previous ban on alcohol advertising in places where its sales or
consumption were prohibited, such as football stadia.
Two years later, the Ministry of Health gave an award to the Federation of Spirits
Producers for its contribution to the National Plan on Drugs.
Alternative scenario
Public-private interactions are likely to grow, and public health authorities and
ocials will have to deal with increasing pressure to engage in collaborations with
corporations responsible for health-damaging products. In the case study described
above, the Public Health Directorate recognised that any trade organisation was free
to adopt self-regulation for issues not covered by legal regulations, and knew that
the Ministry should not be involved as this might prevent the enactment of formal
and stricter rules. The outcome of the case study shows that policies that are linked
too closely to individuals may be short-lived. Instead of taking decisions on a case-
by-case basis, an alternative scenario would be to pre-empt proposals by reinforcing
permanent institutional procedures and structures, based on a framework to guide
health policy-making. The design and implementation of procedures that combine
ethical and good governance issues could help in creating a lasting institutional
culture that prevents interactions that may harm public health.
100
Public health and the food and drinks industry: The governance and ethics of interactionCASE 9: Spain
Discussion
Case questions
1 Do we have to avoid any interaction with corporations that manufacture health-promoting
products because they also manufacture harmful products?
2 Do severe budgetary restrictions warrant supporting public-private interactions that
provide additional funding and expertise to implement health promotion activities?
Nowadays, it is easy to agree that any collaboration with the tobacco industry
should be avoided. However, there is a grey area between alcohol and clearly health-
promoting services or products. The ethical code adopted by the American Public
Health Association (Thomas et al, 2002) states that public health institutions and
their employees should engage in collaborations and aliations in ways that build the
public’s trust and the institution’s eectiveness. However, some guidance is needed to
assess trust and eectiveness. Five tests have been proposed for public policy-makers
when considering any such public-private partnership (Galea and McKee, 2014). The
rst and most important test concerns the potential of the products and services of
the companies involved to enhance or damage health. In this respect, although we
have no doubt regarding the inappropriateness of interacting with alcohol producers,
we feel that interactions with some food and drink companies may raise doubts.
When doubts arise about the wisdom of engaging with alcohol companies, we need
to consider whether the companies explicitly recognise the harms caused by their
products or whether they are promoting new strategies of packaging and marketing
that clearly target vulnerable populations. The second test is a check on the behaviour
of the private partner in their own workplaces. The third examines transparency and
the external assessment of corporate social responsibility programmes. The fourth
questions the extent to which corporations make contributions to the common good,
and the fth relates to the role that corporations should be allowed to play in the
policy process. In our view, the application of these tests requires an extension of
public health surveillance activities in order to monitor corporate practices and ensure
that the corporations know they are under observation. Regarding participation in
the policy process, corporations might be consulted but not invited to join the policy
formulation process. The contribution to the consultation process should respect
the equity principle, which means that population groups representing the more
disadvantaged sectors should be given more time and voice.
The current economic crisis appears to be long-lasting and it is unlikely that public
health budgets will increase greatly in the near future. This generates the permanent
temptation to engage in public-private interactions, with the hope that the resources
or expertise obtained will result in more benets than harm. In particular situations
such as public health crises, the oer of collaboration is readily welcome, but we
101
Public health and the food and drinks industry: The governance and ethics of interaction CASE 9: Spain
must be aware and vigilant of potential risks. For example, the oer of a third of the
surface of a can of a sweetened beverage to include a health message is appealing
when you have severe budget restrictions, but should we agree to display the
logo of a government health department on soft drink cans (Hernández-Aguado
and Lumbreras, 2016)? Budgetary restrictions are not enough to justify such
collaboration. The question is how to mitigate the risks. Public health institutions
and practitioners should be well equipped with ethical principles and guidelines
for governance of public-private interactions. Just as other codes are naturally
incorporated in any public health intervention, it is essential to develop tools and
procedures that embody ethics and good governance and that can be applied
systematically and routinely to public-private initiatives.
Acknowledgments
We thank Jonathan Whitehead for language editing.
Declarations of interests
Ildefonso Hernández-Aguado
Pharmaceutical
: The Dr Antonio Esteve Foundation and the Víctor Grífols i Lucas Foundation:
I have received fees: 1) as editor of the book:
Priorities in health policy
(Dr Antonio Esteve Foundation, 2016); and
2) for writing a chapter on research priorities in the book
Ethics, health and waste of knowledge
, and a chapter on population most
vulnerable to crisis in the book
Ethics and public health in times of crisis
(The Víctor Grífols i Lucas Foundation, 2015 and 2014).
Joan R Villalbí
None declared.
References
Córdoba R, Villalbí JR, Salvador T, López V (2006). El proceso para la adopción de una legislación eficaz en la prevención del
tabaquismo en España.
Revista Española de Salud Pública
, 80 (6): 631-45.
Galea G, McKee M (2014). Public-private partnerships with large corporations: setting the ground rules for better health.
Health
Policy,
115 (2-3): 138-40.
Hernández-Aguado I (2013). The tobacco ban in Spain: how it happened, a vision from inside the government.
Journal of
Epidemiology and Community Health
, 67 (7): 542-43.
Hernández-Aguado I, Lumbreras B (2016). Public-private partnerships: role of corporate sponsorship in public health. In: Drue
H, Barrett LH, Ortmann AD, et al (2016).
Public Health Ethics: Cases Spanning the Globe
: 80-83. http://link.springer.com/
book/10.1007/978-3-319-23847-0
Nuffield Council on Bioethics (2007). Public health: ethical issues. http://nuffieldbioethics.org/wp-content/uploads/2014/07/Public-
health-ethical-issues.pdf
Rodriguez-Martos A (2007). ¿Por qué es tan difícil legislar sobre alcohol en España?
Adicciones
, 19 (4): 325-31.
Sarasa-Renedo A, Sordo del Castillo L, Molist G, et al (2014). Principales daños sanitarios y sociales relacionados con el consumo
de alcohol.
Revista Española de Salud Pública
, 88 (4): 469-91.
Sureda X, Villalbí JR, Espelt A, Franco M (2017). Living under the influence: normalisation of alcohol consumption in our cities.
Gaceta Sanitaria
, 31: 66-68.
Thomas JC, Sage M, Dillenberg J, Guillory VJ (2002). A code of ethics for public health.
American Journal of Public Health
, 92 (7):
1057-59.
Villalbí JR, Granero L, Brugal MT (2008). Políticas de regulación del alcohol en España: ¿salud pública basada en la experiencia?
Informe SESPAS 2008.
Gaceta Sanitaria
, 22 (Supl 1): 79-85.
Villoria M, Revuelta A (eds) (2014).
An Evaluation of Lobbying in Spain. Analysis and Proposals.
Madrid: Transparency International
España: 80-81. http://webantigua.transparencia.org.es/estudio_lobby/spain_lobbying_english_final.pdf
102
Public health and the food and drinks industry: The governance and ethics of interaction
CASE 10: Global
Health Council
Authors
Craig W Moscetti
Manager, Pediatric
Health Community
Programs, Allina
Health and
HealthPartners, Inc.,
USA
Allyn L Taylor
Affiliate Professor
of Law, University of
Washington School
of Law, USA
Adjunct Professor
of International
Relations, John
Hopkins University
Paul H Nitze School
of Advanced
International Studies,
USA
Corresponding
author
Craig W Moscetti
Email: cwmoscetti@
gmail.com
Summary
In 2010, the Global Health Council (GHC) launched the NCD (Non-
Communicable Diseases) Roundtable – a coalition aimed at elevating NCDs
on the global health agenda. In line with broader sentiment current at the
time towards multi-sector partnerships, the GHC courted new members for
the group, particularly private sector companies. Many took advantage of the
opportunity, including Coca-Cola and PepsiCo.
While partnerships with industry are often welcomed, they come with risks to
public health, particularly those involving food and beverage companies, such
as Coca-Cola, PepsiCo and others, that produce and market products known
to be antithetical to health.
Including food industry partners in this way undermined the GHC with
respect to NCDs in two ways: the Roundtable’s governance, and subsequent
policy recommendations. Under the GHC’s name, Coca-Cola and PepsiCo
participated in the 2011 World Health Assembly, the United Nations High-level
Meeting (HLM), and the Civil Society Consultation Hearing that preceded the
UN HLM. GHC events on global NCDs similarly legitimised PepsiCo and Coca-
Cola as sponsors and prominent speakers and further facilitated their access
to government ocials. And the Roundtable’s recommendations endorsed
inclusive ‘whole-of-society’ approaches to address NCDs, focusing on
voluntary approaches, even with their documented shortcomings, while omitting
regulatory approaches, despite their known ecacy.
The involvement of Coca-Cola and PepsiCo raises important questions as to
whether their contributions to the NCD Roundtable, and to NCD policy dialogue
more generally, were genuine, or merely a calculated strategy to leverage GHC’s
open-door policy with the private sector to create an image of goodwill.
From participation to power: how the sugar-
sweetened beverage industry shapes policy
through multi-stakeholder coalitions
10
CASE

103
Public health and the food and drinks industry: The governance and ethics of interaction
CASE 10: Global
Health Council
Introduction
Long a recognised scourge of high-income countries, non-communicable diseases
(NCDs) are now considered global public health and economic crises. Following
decades of insucient attention, the 2011 United Nations High-level Meeting (HLM)
on Non-communicable Diseases injected much-needed urgency and direction.
The meeting’s Political Declaration established the mandate and agenda for future
governmental and inter-governmental actions, including ‘whole-of-government’
and ‘whole-of-society’ approaches. Inclusive strategies became a unifying theme
and, aside from the tobacco and rearms industries, all stakeholders were deemed
legitimate partners in the eort to combat NCDs (United Nations, 2011).
Such inclusive approaches to combat NCDs – including, in particular, cooperation
and coordinated eorts with the food and beverage industry – have come amidst
a sea change in global health governance. In the 1980s, a new ‘get things done’
sentiment replaced disillusionment in traditional approaches and mistrust of the
private sector. A more favourable view of industry emerged, marked for its potential
to help address critical market failures in an increasingly interdependent world (Buse
and Walt, 2000). A new wave of public-private partnerships (PPPs) ensued (Buse
and Harmer, 2004), and now PPPs command signicant support and power in
global health.
Faced with signicant resource shortfalls and unprecedented complexity, many
view PPPs and other collaborations with industry as key tools to combat NCDs.
Unlike the favourable economic environment of the early 2000s, which saw
unprecedented global health funding growth, governments today face greater
nancial pressures. And with an economic price tag of some US$ 47 trillion over
the coming two decades for inaction towards NCDs, few believe that the public
sector alone can foot the bill (Bloom et al, 2011; Dieleman et al, 2016a; Dieleman
et al, 2016b). Instead, many see opportunity in the private sector’s unique assets
and resource potential, such as global supply chains, marketing prowess, and
research and development capacity (Sturchio and Goel, 2012). After all, business
already commands a signicant presence in developing countries with foreign
direct investments exceeding ocial development assistance for health by 25 times
(Sidibé, 2015).
While partnerships with industry are often welcomed, they come with risks to public
health, particularly those involving food and beverage companies (Taylor et al,
2016). Coca-Cola, PepsiCo and others produce and market products known to be
antithetical to health. Research consistently links consumption of sugar-sweetened
beverages (SSBs) and other sugary products to obesity, metabolic syndrome,
cardiovascular disease and type 2 diabetes (Malik et al, 2010; Stanhope et al, 2015).

104
Public health and the food and drinks industry: The governance and ethics of interaction
Furthermore, SSB consumption is predicted both to expand in developing countries
and to cause a considerable proportion of incident disease (Taylor and Jacobson,
2016; Imamura et al, 2015). At the same time, such companies are known to
employ deceptive tactics to distort science, muddle public perception, and inuence
policy in its favour (Kearns et al, 2016). Between 2011 and 2015, Coca-Cola and
PepsiCo funded nearly 100 dierent health organisations, including those charged
with setting public health norms and standards, while at the same time lobbying
against 29 dierent pieces of public health legislation (Aaron and Siegel, 2017). In
the case of Coca-Cola, this amounted to more than US$ 130 million between 2010
and 2015 (Douglas, 2016). Many of these sponsorships strategically supported
researchers, dietitians and organisations that drew supportive conclusions for
industry, establishing grounds to refute stricter policy measures (New York Times,
2015; Bes-Rastrollo et al, 2013; Choi, 2016; International Council of Beverage
Associations, 2015).
This case study examines the role that major food and beverage companies played
within the Global Health Council’s NCD Roundtable to inuence global NCD policy
at the UN HLM and the World Health Organization (WHO). Furthermore, it oers
important governance lessons for other multi-stakeholder platforms to consider,
especially those engaging with the private sector.
Case
Since 1972, the Global Health Council (GHC) has served as one of global health’s
preeminent civil society voices dedicated to “improve[ing] health globally through
increased investment, robust policies, and the power of the collective voice” (Global
Health Council, 2015). Its membership numbers thousands of organisations,
research entities, businesses and individuals spanning some 150 countries, all
advocating for a shared global health vision under GHC. This broad-based coalition
aords GHC unparalleled legitimacy as a convener and representative of civil society
interests. As such, the organisation maintains distinct pathways for itself and its
members to directly engage in global health policy-making at the highest levels,
such as through its ocial relations status with the World Health Organization,
accreditation with the Economic and Social Council of the UN, and long-standing
relationships across the US government. When fully realised, these assets have put
GHC in many of global health’s most consequential discussions, including the UN
HLM on HIV/AIDS and the annual US government appropriations for the President’s
Emergency Plan for AIDS Relief.
In 2010, GHC launched the Roundtable, a coalition aimed at elevating NCDs on the
global health agenda. Paralleling broader sentiment towards inclusive partnerships
CASE 10: Global
Health Council

105
Public health and the food and drinks industry: The governance and ethics of interaction
(OHCHR et al, 2013), the group courted new members, particularly private sector
companies. Many took advantage of the opportunity, including Coca-Cola and
PepsiCo, whose membership in GHC and participation in the Roundtable intensied
leading up to the UN HLM, only to cease soon after the historic meeting (Moscetti,
2014).
Inclusivity, which historically legitimised the GHC, undermined it with respect
to NCDs in two ways: the Roundtable’s governance, and subsequent policy
recommendations. By granting equal voice to all stakeholders regardless of
interests, objectives clashed. How should the organisation treat prospective or
current members with product lines that undermine health, such as Coca-Cola and
PepsiCo? On the one hand, it could strictly uphold part of the organisation’s mission
to “improve health globally”, or it could focus on the other part of the organisation’s
mission: “increased investment, robust policies and the power of the collective voice.”
Choosing the latter, Coca-Cola and PepsiCo participated under GHC’s name in
the 2011 World Health Assembly, the UN HLM, and the Civil Society Consultation
Hearing that preceded the UN HLM. GHC events on global NCDs similarly
legitimised PepsiCo and Coca-Cola as sponsors and prominent speakers and
further facilitated their access to government ocials (Global Health Council, 2010).
Regarding the Roundtable’s policy recommendations, Coca-Cola, PepsiCo and
the other 80-plus participating organisations could inform and endorse these
recommendations, which GHC subsequently used as its ocial positions to lobby
government ocials involved in negotiating global NCD policy (Global Health
Council, 2011). Reecting the group’s inclusive ethos, these recommendations
endorsed “multi-sector partnerships” and “whole-of-society” approaches to address
NCDs. They focused on voluntary approaches, even given their documented
ineectiveness (Moodie et al, 2013), while omitting regulatory approaches, despite
their known ecacy (Batis et al, 2016; World Health Organization, 2016) and
support among other NCD-focused civil society coalitions (NCD Alliance, 2011).
Furthermore, private business was cast as an important funding source, although
evidence similarly raises questions on whether such funds can produce unbiased
research and programming (Bes-Rastrollo et al, 2013).
The Political Declaration mirrored the heightened value of inclusivity within global
health. “Multi-sectoral” appears in the Political Declaration 15 times, and “whole-of-
government” and “whole-of-society” actions received its own designated section,
the latter implying partnerships with food and beverage companies, who evaded a
“conict of interest” label from member states (United Nations, General Assembly,
2011).
CASE 10: Global
Health Council

106
Public health and the food and drinks industry: The governance and ethics of interaction
Soon after the UN HLM, Coca-Cola and PepsiCo’s participation in the NCD
Roundtable diminished and neither are currently members. This ‘ash in the pan’
engagement by Coca-Cola and PepsiCo raises important questions as to whether
their contributions to the NCD Roundtable, and to NCD policy dialogue more
generally, were genuine, or merely a calculated strategy to leverage GHC’s open-
door policy with the private sector to create an image of goodwill.
GHC was not the sole proponent for inclusive approaches, nor was it the sole
reason the Political Declaration ultimately reected this sentiment. But the case
of the NCD Roundtable raises important questions for other multi-stakeholder
arrangements to ask when considering how their governance and stakeholder rules
of engagement may shape the recommendations they produce.
Alternative scenario
Transparency
Could more stringent disclosure policies better reveal potential conicts of interest?
Proponents believe transparency roots out conicts of interest (Ru, 2015), while
others argue it is still insucient (Nestle, 2016). While the NCD Roundtable disclosed
its membership in some instances, such as on policy documents and with event
sponsors, transparency fell short in others. Few will argue that greater transparency
can help manage actual or perceived conicts of interest when developing NCD-
related policies, as a recent Congressionally mandated review of the Dietary
Guidelines for Americans process found (National Academy of Science, 2017).
Partitioning ‘civil society’
One way to improve transparency is through further partitioning civil society.
Aording equal voice to business and other segments of civil society masks
interests. And across what is commonly referred to as ‘civil society’, interests vary
greatly. For example, publicly traded corporations hold dierent nancial duties from
not-for-prot charitable organisations. As such, coalitions might partition business
from the rest of civil society, especially in the context of agenda-, policy-, or norms-
setting.
CASE 10: Global
Health Council
107
Public health and the food and drinks industry: The governance and ethics of interaction
107
Public health and the food and drinks industry: The governance and ethics of interaction
Discussion
Case question
Given the consistent and extensive research showing the harmful health effects of
consumption of sugar-sweetened beverages (SSBs) in children and adults, should the public
sector engage in partnerships with SSB companies like Coca-Cola and PepsiCo? If so, what
ground rules should apply to such partnerships?
Although politically appealing, unchecked collaboration with food and beverage
companies carries considerable risk to the protection of the public’s health.
Principally, are they trusted partners? Do industry self-regulation and PPPs improve
public health, or are they “public relations and market expansion gambits for the
private sector,” as was once stated (Ng and Ruger, 2011)? To date, evidence
supports less of the former and more of the latter. PPPs to advance health have
shown mixed results, and voluntary industry approaches across tobacco, alcohol,
and ultra-processed food and beverage industries have likewise come up short
(Hernandez-Aguado and Zaragoza, 2016; Kunkel et al, 2015; Moodie et al, 2013).
Improvements under Walmart’s Healthier Food Initiative, for example, simply
“mirror[ed] preexisting trends” (Taillie et al, 2015). The Healthy Weight Commitment
Foundation removed a relatively modest number of per capita calories from the
US food supply over ve years, the equivalent of six ounces of Coca-Cola (Ng et
al, 2014). Improvements in food marketing to children similarly lag behind stated
commitments (Hawkes and Harris, 2011; Kunkel et al, 2015).
While public health ultimately bears the risk and cost for failed industry collaborations,
industry reaps the benet of increased trust and legitimacy. NCDs persist as public
health threats, exacerbated by industry in some cases (GBD 2015 Risk Factors
Collaborators, 2016). Yet industry is increasingly welcomed into global partnerships. Look
no further than former First Lady Michelle Obama’s praise for the Healthy Weight Commitment
Foundation’s results to see the public relations upside for industry (Kass, 2014).
Deploying tobacco-industry-like tactics, “the food industry is ripe for scrutiny” (PLoS
Medicine Editors, 2012). PPPs can advance progress towards development goals,
but “are not automatically the right choice to solve every challenge” (Ferroni and
Castle, 2011). Full participation of all interests should not be assumed. Rather, roles
should be carefully questioned, and explicitly dened and made fully transparent,
particularly those with food and beverage companies. Is their involvement to protect
public health, or to strategically full business interests (Hawkes and Buse, 2011)?
Multi-stakeholder approaches, pursued by WHO or otherwise, should dene clear
terms of engagement, and deploy sucient monitoring, accountability and risk-
management controls to safeguard public health.
CASE 10: Global
Health Council

108
Public health and the food and drinks industry: The governance and ethics of interaction
CASE 10: Global
Health Council
Declarations of interests
Craig W Moscetti
None declared.
Allyn L Taylor
None declared.
References
Aaron D, Siegel M (2017). Sponsorship of national health organizations by two major soda companies.
American Journal of
Preventive Medicine
, 52 (1): 20-30. doi: 10.1016/j.amepre.2016.08.010
Batis C, Rivera J, Popkin B, Taillie L (2016). First-year evaluation of Mexico’s tax on nonessential energy-dense foods: an
observational study.
PLoS Medicine
, 13 (7): e1002057. doi: 10.1371/journal.pmed.1002057
Bes-Rastrollo M, Schulze MB, Ruiz-Canela M, Martinez-Gonzalez MA (2013). Financial conflicts of interest and reporting bias
regarding the association between sugar-sweetened beverages and weight gain: a systematic review of systematic reviews.
PLoS
Medicine,
10: e1001578. doi: 10.1371/journal.pmed.1001578
Bloom D, Cafiero E, Jané-Llopis E, et al (2011).
The Global Economic Burden of Noncommunicable Diseases.
Geneva: World
Economic Forum.
Buse K, Harmer A (2004). Power to the partners? The politics of public-private health partnerships.
Development
, 47 (2): 49-56. doi:
10.1057/palgrave.development.1100029
Buse K, Walt G (2000). Global public-private partnerships: part I – a new development in health?
Bulletin of the World Health
Organization
, 78(4): 549-61.
Choi C (2016). Soda group suspends payments to dieticians opposing new tax.
ABC News
, 6 October 2016.
Dieleman J, Schneider M, Haakenstad A, et al (2016a). Development assistance for health: past trends, associations, and the future
of international financial flows for health.
Lancet
, 387 (10037): 2536-44. doi: 10.1016/S0140-6736(16)30168-4
Dieleman J, Templin T, Sadat N, et al (2016b). National spending on health by source for 184 countries between 2013 and 2040.
Lancet
, 387 (10037): 2521-35. doi: 10.1016/S0140-6736(16)30167-2
Douglas S (2016). Our actions and way forward. The Coca-Cola Company, 24 March 2016. http://transparency.coca-colacompany.
com/
Ferroni M, Castle P (2011). Public-private partnerships and sustainable agriculture development.
Sustainability
, 3 (7): 1064-73. doi:
10.3390/su3071064
GBD 2015 Risk Factors Collaborators (2016). Global, regional, and national comparative risk assessment of 79 behavioral,
environmental and occupational, and metabolic risk or cluster of risks, 1990-2015: a systematic analysis for the Global Burden of
Disease Study 2015.
Lancet
, 388 (10053): 1659-1724. doi: 10.1016/S0140-6736(15)00128-2
Global Health Council (2010).
Building Multi-Stakeholder Partnerships for NCDs: Ideas, Steps and Actions
. Washington, DC:
Global Health Council. http://globalhealth.org/wp-content/uploads/ghc_Multi-stakeholder-engagement-for-NCDs_final.pdf
Global Health Council (2011).
Global Leadership, Local Solution: Mobilizing for NCDs
. Washington, DC: Global Health Council.
https://issuu.com/globalhealthcouncil/docs/ncds
Global Health Council (2015). About us. http://globalhealth.org/about-us/mission-and-vision/ [Accessed 6 February 2017.]
Hawkes C, Buse K (2011). Public health sector and food industry interaction: it’s time to clarify the term ‘partnership’ and be honest
about underlying interests.
European Journal of Public Health
, 21 (4): 400-01. doi: 10.1093/eurpub/ckr077
Hawkes C, Harris J (2011). An analysis of the content of food industry pledges on marketing to children.
Public Health Nutrition
, 14
(8): 1403-14. doi: 10.1017/S1368980011000607
Hernandez-Aguado I, Zaragoza G (2016). Support of public-private partnerships in health promotion and conflicts of interest.
BMJ
Open
, 6: e009342. doi: 10.1136/bmjopen-2015-009342
Imamura F, O’Connor L, Ye Z, et al (2015). Consumption of sugar sweetened beverages, artificially sweetened beverages, and fruit
juice and incidence of type 2 diabetes: systematic review, meta-analysis, and estimation of population attributable fraction.
British
Medical Journal
, 351: h3576. doi: 10.1136/bmj.h3576
International Council of Beverage Associations (2015). Statement on WHO Guideline: Sugars intake for adults and children.
http://www.icba-net.org/files/resources/icbawhosugarpressstatementfinal.pdf

109
Public health and the food and drinks industry: The governance and ethics of interaction
CASE 10: Global
Health Council
Kass S (2014). Through commitment with the Partnership for a Healthier America, Healthy Weight Commitment Foundation
members exceed their calorie reduction goal by 400%. Let’s Move Blog, 9 January 2014. https://letsmove.obamawhitehouse.
archives.gov/blog/2014/01/09/through-commitment-partnership-healthier-america-healthy-weight-commitment-foundatio
Kearns C, Schmidt L, Glantz S (2016). Sugar industry and coronary heart disease research: a historical analysis of internal industry
documents.
JAMA Internal Medicine
, 176 (11): 1680-85. doi: 10.1001/jamainternmed.2016.5394
Kunkel D, Castonguay J, Filer C (2015). Evaluating industry self-regulation of food marketing to children.
American Journal of
Preventive Medicine
, 49 (2): 181-87. doi: 10.1016/j.amepre.2015.01.027
Malik V, Popkin B, Bray G, et al (2010). Sugar-sweetened beverages and risk of metabolic syndrome and type 2 diabetes: a meta-
analysis.
Diabetes Care
, 33 (11): 2477-83. doi: 10.2337/dc10-1079
Moodie R, Stuckler D, Monteiro C, et al (2013). Profits and pandemics: prevention of harmful effects of tobacco, alcohol, and ultra-
processed food and drink industries.
Lancet
, 381: 670-79. doi: 10.1016/S0140-6736(12)62089-3
Moscetti C (2014). Moscetti C, NCD Roundtable Chair in 2011. Personal communication.
National Academy of Science, Health and Medicine Division, Food and Nutrition Board (2017).
Optimizing the Process for
Establishing the Dietary Guidelines for Americans: The Selection Process
. Washington, DC: The National Academies of Sciences,
Engineering, and Medicine. https://www.nap.edu/catalog/24637/optimizing-the-process-for-establishing-the-dietary-guidelines-
for-americans
NCD Alliance (2011).
Proposed Outcomes Document for the United Nations High-Level Summit on Non-Communicable Diseases
.
https://ncdalliance.org/sites/default/files/resource_files/NCD%20Alliance%20Proposed%20Outcomes%20Document%20
for%20the%20UN%20High-Level%20Summit.pdf
Nestle M (2016). Corporate funding of food and nutrition research: science or marketing?
JAMA Internal Medicine
, 176 (1): 13-14.
doi:10.1001/jamainternmed.2015.6667
New York Times (2015). Coca-Cola funds scientists who shift blame for obesity away from bad diets.
New York Times
, 9 August
2015. http://well.blogs.nytimes.com/2015/08/09/coca-cola-funds-scientists-who-shift-blame-for-obesity-away-from-bad-diets/
Ng NY, Ruger JP (2011). Global health governance at a crossroads.
Global Health Governance
, 3 (2): 1-37.
Ng S, Slining M, Popkin B (2014). The Healthy Weight Commitment Foundation pledge: Calories sold from U.S. consumer
packaged goods, 2007-2012.
American Journal of Preventive Medicine
, 47 (4): 508-19. doi:10.1016/j.amepre.2014.05.029
OHCHR, UNEP, UNFPA, WHO (2013).
Partnerships for development: Perspectives from global health. Thematic Think Piece, UN
System Task Team on the Post-2015 UN Development Agenda
. http://www.un.org/en/development/desa/policy/untaskteam_undf/
thinkpieces/25_thinkpiece_health.pdf
PLoS Medicine Editors (2012). PLoS Medicine Series
on Big Food: the food industry is ripe for scrutiny.
PLoS Medicine
, 9 (6):
e1001246. doi:10.1371/journal.pmed.1001246
Ruff K (2015). Scientific journals and conflict of interest disclosure: what progress has been made?
Environmental Health
, 14: 45.
doi:10.1186/s12940-015-0035-6
Sidibé M (2015). Why we need the private sector and why it needs us: governing global health differently post-2015.
Global Health
and Diplomacy
. http://onlinedigeditions.com/article/Why_ We_Need_The_Private_Sector_And_Why_It_Needs_Us%3A_
Governing_Global_Health_Differently_Pos t-2015/1910242/242901/article.html
Stanhope K, Medici V, Bremer A, et al (2015). A dose-response study of consuming high-fructose corn syrup-sweetened beverages
on lipid / lipoprotein risk factors for cardiovascular disease in young adults.
American Journal of Clinical Nutrition
, 101 (6):
1144-54. doi:10.3945/ajcn.114.10061
Sturchio J, Goel A (2012).
The Private-Sector Role in Public Health: Reflections on the New Global Architecture in Health
.
Washington, DC: Center for Strategic and International Studies.
Taillie LS, Ng SW, Popkin BM (2015). Gains made by Walmart’s healthier food initiative mirror preexisting trends.
Health Affairs
, 34
(11): 1869-76. doi:10.1377/hlthaff.2015.0072
Taylor A, Jacobson M (2016).
Carbonating the World: The Marketing and Health Impact of Sugar Drinks in Low- and Middle-income
Countries
. Washington, DC: Center for Science in the Public Interest.
Taylor R, Amankwah F, Nalamada P (2016).
Engaging the Private Sector and Developing Partnerships to Advance Health and the
Sustainable Development Goals: Proceedings of a Workshop
–
In Brief.
Washington, DC: The National Academies Press.
United Nations, General Assembly (2011).
Political declaration of the High-level Meeting of the General Assembly on the Prevention
and Control of Non-communicable Diseases (A/66/L.1)
. http://www.un.org/ga/search/view_doc.asp?symbol=A/66/L.1
World Health Organization (2016).
Fiscal Policies for Diet and Prevention of Noncommunicable Diseases, Technical Meeting Report
.
Geneva: WHO. http://apps.who.int/iris/bitstream/10665/250131/1/9789241511247-eng.pdf?ua=1
110
Public health and the food and drinks industry: The governance and ethics of interactionCASE 11: England
Authors
Clare Panjwani
Centre for Food
Policy, City, University
of London, UK
Martin Caraher
Professor of
Food and Health
Policy, Centre for
Food Policy, City,
University of London,
UK
Corresponding
author
Martin Caraher
Email: m.caraher@
city.ac.uk
Note
This case study is
based on: Panjwani
C, Caraher M (2014).
The Public Health
Responsibility Deal:
brokering a deal for
public health, but on
whose terms?
Health
Policy
, 114 (2): 163-
73. doi: 10.1016/j.
healthpol.2013.
11.002
A copyright-free
version of the
original research
can be found at
http://open
access.city.ac.uk/
2878/
Summary
Coalitions of multi-national food and drink businesses – sometimes called ‘Big
Food’ – have entered into partnerships with governments and civil society,
pledging to reformulate their products and to market them responsibly. Largely
business-led and self-regulated, the integrity of these voluntary initiatives has
been questioned. The Public Health Responsibility Deal in England (Department
of Health, 2015a) is an example of a voluntary initiative that is government-
led. Does this approach provide evidence that with public leadership there is
potential for voluntary actions to deliver meaningful results for public health?
The focus of this case study is the calorie reduction initiative of the Public Health
Responsibility Deal. Source material was obtained primarily through a series
of UK Freedom of Information requests and comprises previously unpublished
Department of Health documentation relating to relevant meetings held during
2011 and 2012.
The Responsibility Deal approach to calorie reduction deliberately involves
the food industry in the specication of the measures it is to implement
(reformulation and portion control). Finding the common ground between private
and public interests has resulted in the deection of public health objectives and
the preclusion of adequate monitoring and evaluation.
The Responsibility Deal approach is fundamentally awed in its expectation that
industry will take voluntary actions that prioritise public health interests above
its own. Being government-led counts for little in the absence of sanctions to
drive compliance. Instead, the initiative aords private interests the opportunity
to inuence, in their favour, public health policies and strategies that aect their
products.
Voluntary agreements and the power of the food
industry: the Public Health Responsibility Deal
in England
11
CASE

111
Public health and the food and drinks industry: The governance and ethics of interaction CASE 11: England
Introduction
As public-private partnerships become more common and governments see them
as a way out of enforcing regulation, there is a need to examine in detail the various
initiatives in operation (Buse and Harmer, 2007). In neo-liberal market economies
there are arguments for industries to be only lightly regulated and for consumers
to be free to exercise choice. This case study sets out research carried out on the
Public Health Responsibility Deal for England. Between March 2011 and June 2013,
the Food Network of the Responsibility Deal developed pledges that addressed
out-of-home calorie labelling, trans fat removal, salt reduction, fruit and vegetable
promotion, and calorie reduction. The focus of our research was the calorie
reduction pledge element of the Responsibility Deal.
The Public Health Responsibility Deal was launched in England in March 2011
and represented a partnership approach to public health whereby government
engaged with private sector and non-governmental organisation partners in eorts
to address public health objectives. The calorie reduction initiative was notable for its
ambition to drive the national obesity target in England towards “a downward trend
in the level of excess weight averaged across all adults by 2020”. This was to be
achieved by reducing the nation’s collective calorie intake by ve billion calories per
day – equivalent to 100 calories per person per day and an estimate of the average
reduction necessary to achieve a healthy weight. Responsibility Deal partners
were supposed to pledge to reduce calories through reformulation and portion-
size reduction of products, and by encouraging behavioural change in consumers
through activities such as the promotion of smaller portion sizes or making healthier
products available. This approach, inuenced by behavioural science theories (Thaler
and Sunstein, 2008), aimed to make the existing, default choice the lower-calorie
choice (as opposed to oering lower-calorie alternatives), thus ‘nudging’ consumers
towards reduced calorie consumption.
Case
Our work investigated the potential impact of private sector engagement in public
health by looking at a working example: the Public Health Responsibility Deal in
England. The Responsibility Deal was organised into ve networks, each with a
specic focus: food, alcohol, physical activity, health at work and behaviour change.
Partner organisations pledged voluntary actions, agreed by the networks, which
were designed to help meet public health goals. In terms of actors, Figure 1 shows
the key players at the time of the research, along with those who, later in the
process, withdrew from the negotiations.
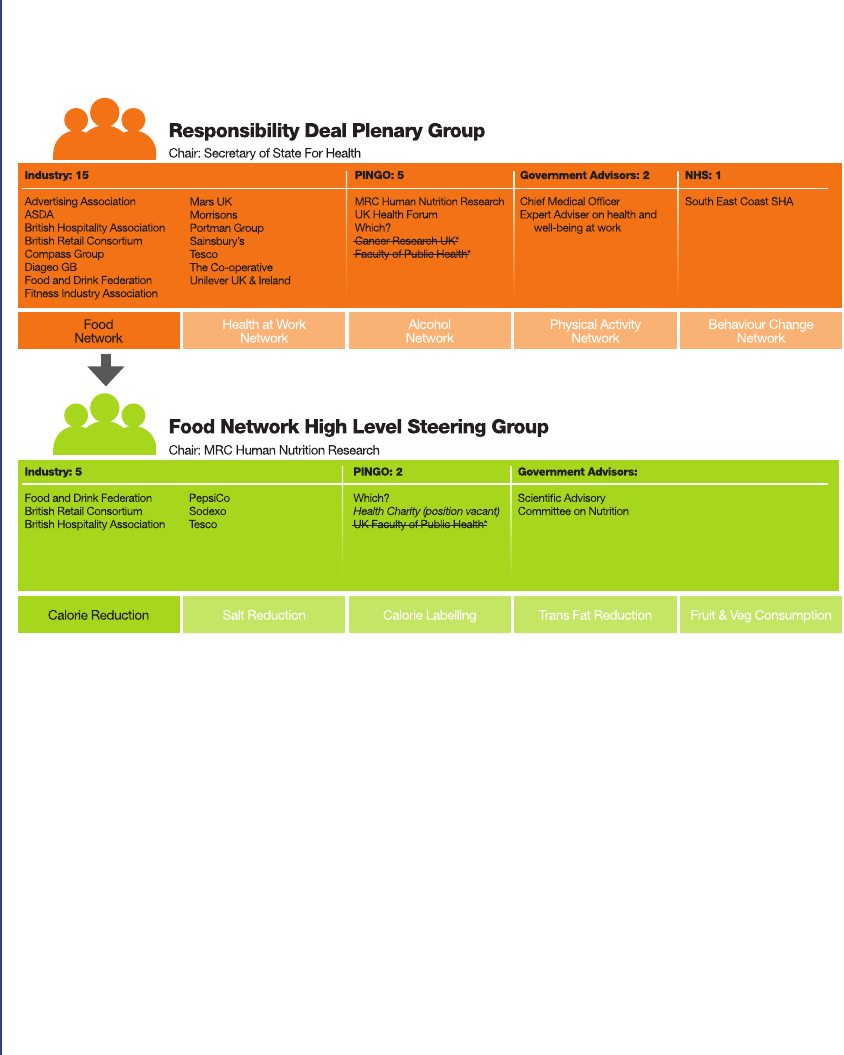
CASE 11: England
112
Public health and the food and drinks industry: The governance and ethics of interaction
Figure 1: Organisational structure and membership of the Responsibility Deal and Food
Network at July 2013
Strike-throughs show those organisations that withdrew.
*July 2013 – Withdrew citing
prioritisation of industry interests in
formulation of gov alcohol strategy.
*July 2013 – Withdrew citing
prioritisation of industry interests in
formulation of gov alcohol strategy.
Specically, we looked at the Responsibility Deal calorie reduction pledge – its
stakeholder representation, working practices, and development and implementation
– in order to identify the role and inuence of the private sector. The Responsibility
Deal is among several types of voluntary arrangements that have emerged within
the past decade where policy-makers and government administrators have
favoured collaborative, voluntary approaches, as opposed to legislative or regulatory
approaches, to address leading public health problems (Bryden et al, 2013; Kraak
et al, 2012). The arguments in favour of collaboration with industry partners are that
it is more eective than acting independently of them and that it allows practical
actions to be agreed upon more quickly and with less cost than legislation. The
argument against is that the approach aords industry the opportunity to inuence
the development of public health policy to its own ends (Moodie et al, 2013).

CASE 11: England
The methods adopted for our research are set out in the introduction to this case
study, but of note was the fact that the key documents for analysis were obtained
primarily through a series of UK Freedom of Information requests and constituted
previously unpublished Department of Health documentation relating to relevant
meetings held during 2011 and 2012. This was because, at the time of the research,
many of the minutes of meetings and documents were not available on the website.
This can be seen as a lack of transparency and due process. So the changes to the
agreements as set out below were not public knowledge, and were not helped by
the fact that the public health representatives had withdrawn from the negotiations
(see Figure 1 on page 112).
Our ndings exposed serious aws in both the process and the lack of outcome
measures. The key points are:
• The process had left the industry lobby and representatives to rewrite the rules
of the games, with processes and ‘old gains’ being allowed to be included as
indicators of success.
• There were no agreed outcome measures with respect to population-level
outcomes. For example, it was possible to use industry data on packaged
food categories to measure a company’s commitment to a reduction in calories
(Panjwani and Caraher, 2014).
Public health and the food and drinks industry: The governance and ethics of interaction
113
The delivery of public health outcomes was compromised and deected. In many
respects we feel that the industry perspective is not unusual; they are not there to
argue public health at any cost. This corporate capture of public health (Mindell
et al, 2012; Moodie et al, 2013) is epitomised by the Responsibility Deal’s and
the government’s willingness to see voluntary agreements as more desirable than
legislation. Another factor that contributed to the lack of progress was that the UK
Faculty of Public Health withdrew from the Responsibility Deal (see Figure 1 on page
112), due to what they saw as the prioritisation of private interests and a lack of
evidence that the Responsibility Deal was achieving its goal of being faster and more
eective than legislation (Faculty of Public Health, 2013). While understanding their
position, it meant that there was no public health voice at the negotiating table. This
raises ethical issues over the omission of key voices and the withdrawal of public
health advocates from the negotiations.
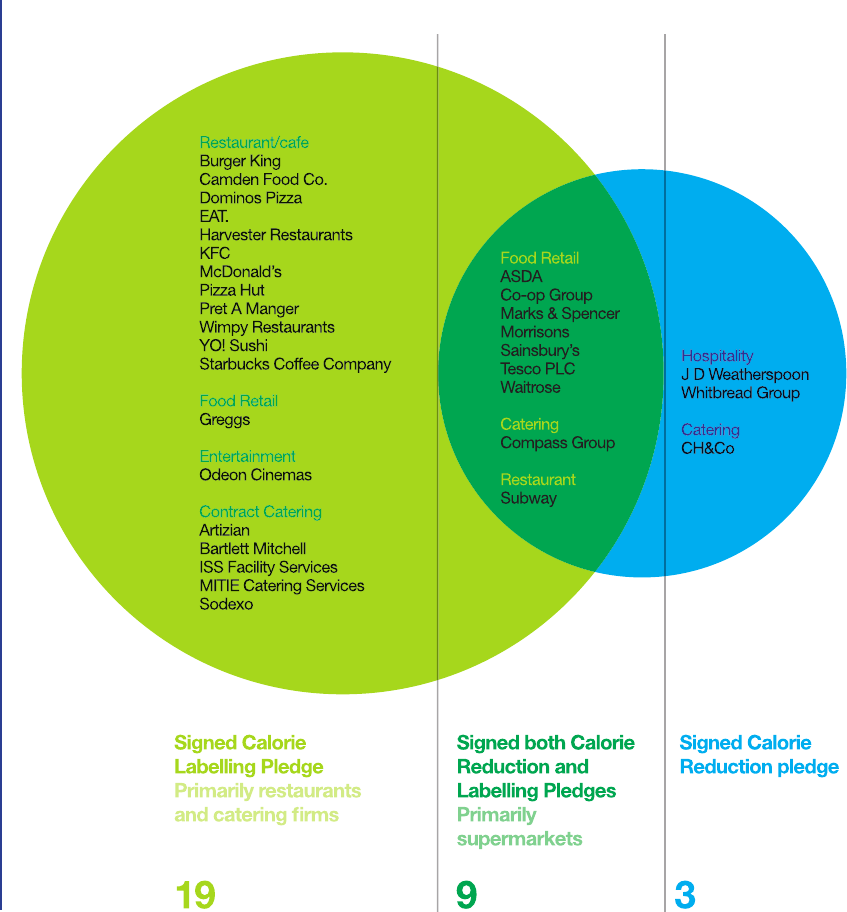
114
Public health and the food and drinks industry: The governance and ethics of interaction
Figure 2: Signatories to the calorie labelling and calorie reduction pledges
CASE 11: England

115
Public health and the food and drinks industry: The governance and ethics of interaction
When the Responsibility Deal was launched, there were 17 signatories representing
the manufacturing, retail and food service sectors. One year after its launch, 29
companies had published a calorie reduction pledge that detailed the actions they
would take. Industry sectors were represented to varying degrees. Large fast food
restaurant chains, for example, are conspicuously absent, despite some being
signatories to other Responsibility Deal pledges. Figure 2 shows that many fast
food and hospitality businesses signed the labelling pledge but not the commitment
to reduce calorie content. This is despite many of those businesses being
characterised by high-calorie, energy-dense foods to which the calorie reduction
pledge would be particularly relevant.
Alternative scenario
The ideal would be that any agreement is enforced by legislation, ensuring public
sign-up by companies and the setting of specic, time-bound outcome targets. This
could include the imposition of penalties for not meeting targets. The private sector
could then seek to distinguish between themselves by setting higher standards for
both food composition and practices. The latter might include commitments not to
market to children.
Our preferred alternative scenario entails mandatory requirements (i.e. the top half
of Figure 3) and a strong recommendation for a move to measure and hold food
manufacturers and retailers to account on the basis of outcomes and not processes.
Any alternative scenario should meet the following criteria:
1 It should not rely on process measures to gauge outcomes.
2 It should draw on conventional public health and alternative sources of data, such
as econometric data, to determine both outcomes and contributions to the burden
of ill health.
3 It should ensure that any agreements are supported by legislation, or at least there
should be penalties for not addressing the outcomes.
Buse and Harmer (2007) usefully identify ‘seven habits’ of eective global public-
private partnerships and, while it is important to establish accountability, monitoring
and enforcement structures in public-private collaborations, they need to be
bounded by clear, non-negotiable issues related to public health outcomes. This is
policy which is a mix of clear legislation and forfeits if targets are not met.
CASE 11: England
116
Public health and the food and drinks industry: The governance and ethics of interaction
Upstream
Downstream
• Regulation
• Mandatory reformulation
• Subsidies and taxation
• Voluntary reformulation eg PPPs
• Nudging
• Labelling
• Media campaigns
• Community and work based dietary interventions
• Clinical dietetics
Evaluation could be carried out at regular intervals and be based on outcomes, and
not solely on process towards achieving targets. So consumption data and health
status could be used as indicators of success. Using the Responsibility Deal to
enforce product reformulation and calorie reduction of products would ensure that
education and relying on consumer choice are not the default option (Oliver, 2011).
The establishment of a separate and independent monitoring agency would add to
the process and introduce a level of independence.
CASE 11: England
Figure 3: Public health levels of intervention
117
Public health and the food and drinks industry: The governance and ethics of interaction CASE 11: England
Discussion
Case questions
1 Should the Responsibility Deal and others like it be scrapped as not fit for purpose?
2 Would the introduction of specific standards or regulations help implementation?
3 What ‘outcome standards’ would help deliver on voluntary promises or agreements?
4 What should public health agencies insist is non-negotiable in terms of public-private
partnerships?
5 At what stage should a public health body withdraw from negotiations (where their
continued presence might lend an air of approval to the proceedings)?
The problem was the ‘pick and choose’ nature of the Responsibility Deal, where
companies could choose initiatives that did not conict with their core business.
There was a failure to hold the food industry to account on the basis of agreed
outcome measures such as reductions at a population level in calorie intake and
obesity rates. The ethics of a situation where the power to set standards and
measures is with the more powerful player is questionable (Telfer, 1996). Additionally,
for policy-makers and researchers there arises an ethical question of basing success
criteria on a procedure that is awed and that uses actions as opposed to outcomes
to indicate success. For the private sector to take meaningful actions that prioritise
public health interests above its own will require considerable incentive. To expect
them to be made voluntarily is misguided. There comes a point where a judgement
has to be made when some initiatives may not be worth engaging with. This is
especially so when the focus and decisions about success are based solely on
processes determined by the industry players (Gomes, 2015).
While this may help explain why public health representatives withdrew from the
negotiations, it does not address the ethics of leaving the discussion with nobody in
place with public health expertise to argue the case. Our research did not address
why this occurred, nor the implications of leaving the table clear for the food industry
to dominate the proceedings. It does raise an interesting conundrum not addressed
in the Nueld Council on Bioethics (2007) document on public health which is:
when, on ethical grounds, an individual or group withdraws from negotiations, what
is their ethical position regarding representing the public interest and the greater
good? The nearest the document comes to covering this is when it says “Because
the need being addressed is an important one, it is desirable to explore the potential
of promising policies, even if evidence for their eectiveness is incomplete” (page
xxv). We do not have an answer to this conundrum, but rather a series of questions:

118
Public health and the food and drinks industry: The governance and ethics of interaction
• At what stage is it justied, on ethical grounds, to withdraw from a process of
negotiation?
• What are the implications of leaving the negotiation table free from public health
interests?
• What is the duty of public health professionals and organisations to the public?
• At what point do public health professionals stop negotiating with Big Food as the
vectors of disease (Gilmore et al, 2011)?
The Responsibility Deal’s voluntary partnership approach is claimed by government
to have achieved more, faster and more cheaply, than regulation (Department of
Health, 2015b). Our research suggests, in contrast, that it is the collaborative,
voluntary working practices of the approach that have undermined its potential as
a public health policy tool and hindered its ability to deliver at a population level.
Our view is that regulation is the way forward to deliver on public health outcomes.
We recognise that this is in contrast to the Nueld Council on Bioethics (2007)
document which states that “[A]lthough the regulation of industry can be necessary,
much can be achieved through industry self-regulation. There are several examples
where voluntary commitments may lead to healthier choices being oered to
consumers.” The Responsibility Deal legitimised industry involvement in the design
of policy measures, with no sanctions or targets to ensure those measures drove
or contributed to public health goals. It aorded private interests the opportunity
to inuence, in their favour, the public health policies and strategies that aect their
products – what has been called by others the corporate capture of public health by
Big Food (Mindell et al, 2012).
Some argue that public-private partnerships can contribute to public health
outcomes (Buse and Harmer, 2007), but Big Food has to deliver what it promises.
Key learning from our research is that business has defaulted on the original
intention, which was not just about having lower-calorie options but was about
shifting the whole oering in a direction that emphasised the provision of information
to consumers. So the pledge to reduce the nation’s collective calorie intake by ve
billion calories per day (Gornall, 2014) – equivalent to 100 calories per person per
day – could be monitored using econometric data and even applied to individual
companies and/or categories of food. Of course no one initiative will deliver on its
own; it needs to be linked with a comprehensive approach which incudes all the
elements in Figure 3. The proposed measurement issue here includes the more
conventional approach argued by colleagues such as Petticrew et al (2013) and
involves using commercial data sources to ensure outcomes are addressed.
CASE 11: England

119
Public health and the food and drinks industry: The governance and ethics of interaction
So: has the industry reduced calories, and has there been a reduction in
overweight? This is fundamentally dierent from measuring process and claiming
that this is eective.
Of course we would expect Big Food to argue its case, but what is more disturbing
is the lack of accountability by ministers and civil servants to argue for the greater
good or to set limits on what is negotiable. Below we summarise some of the
possible ways forward.
Recommended actions to ensure good governance of the calorie reduction
initiative
• Publish a timetable of legislative actions that will be enforced if the initiative does
not meet its ve billion calorie reduction target.
• Instruct an independent review of stakeholder representation and working
practices to ensure that inuence is appropriate and transparent.
• Devise SMART (Specic, Measurable, Attainable, Relevant and Time-bound)
company- and sector-level calorie reduction targets – such as a at rate
percentage calorie reduction target across products of low nutritional value.
The combined targets for each sector should derive from the ve billion calorie
reduction target.
• Monitor population-level outcomes – for example, by monitoring caloric
changes from the supply side (using sales data) and consumption side (using
nutrition data), or by using existing population weight surveys as a proxy
measure for calorie reduction.
Source: Panjwani and Caraher, 2014.
In 2016, the government launched its new childhood obesity strategy, which has
been criticised for its lack of detail (HM Government, 2016). While this contains
some proposed regulation, as in the sugar tax on soft drinks, the strategy reinforces
the concept of working with the food industry to nd ways to make food healthier,
and views many of the solutions within technological xes and working with the
industry by “[H]arnessing the best new technology” and “supporting innovation”.
Hence many of the issues raised above remain pertinent.
CASE 11: England
120
Public health and the food and drinks industry: The governance and ethics of interaction
Declarations of interests
Clare Panjwani
None declared.
Martin Caraher
None declared.
References
Bryden A, Petticrew M, Mays N, et al (2013). Voluntary agreements between government and business – A scoping review of the
literature with specific reference to the Public Health Responsibility Deal.
Health Policy
, 110: 186-97.
Buse K, Harmer A (2007). Seven habits of highly effective global public-private health partnerships: practice and potential.
Social
Science and Medicine
, 64 (2): 259-71.
Department of Health (2015a). Public Health Responsibility Deal. https://responsibilitydeal.dh.gov.uk/
Department of Health (2015b). Partner reception to celebrate achievements.
https://responsibilitydeal.dh.gov.uk/partner-reception-to-celebrate-achievements/
Faculty of Public Health (2013). FPH withdraws from Responsibility Deal. http://www.fph.org.uk/fph_withdraws_from_
responsibility_deals [Accessed 22 July 2013.]
Gilmore AB, Savell E, Collin J (2011). Public health, corporations and the new responsibility deal: promoting partnerships with
vectors of disease?
Journal of Public Health
(Oxf), 33: 2-4.
Gomes FS (2015). Conflicts of interest in food and nutrition.
Cadernos de Saúde Pública
, 31 (10): 2039-46. doi: 10.1590/0102-
311XPE011015
Gornall J (2014). Is the billion unit pledge just window dressing?
British Medical Journal
, 348 (g3190). http://dx.doi.org/10.1136/
bmj.g3190
HM Government (2016).
Childhood Obesity: A Plan for Action
. Crown copyright 2016. Published to gov.uk, in PDF format only.
https://www.gov.uk/government/organisations/department-of-health-and-social-care
Kraak V, Harrigan P, Lawrence M, et al (2012). Balancing the benefits and risks of public-private partnerships to address the global
double burden of malnutrition.
Public Health Nutrition
, 15 (3): 503-17.
Mindell JS, Reynolds L, Cohen DL, McKee M (2012). All in this together: the corporate capture of public health.
British Medical
Journal
, 345: e8082.
Moodie R, Stuckler D, Monteiro C, et al and Lancet NCD Action Group (2013). Profits and pandemics: prevention of harmful effects
of tobacco, alcohol, and ultra-processed food and drink industries.
The Lancet
; 381: 9867: 670-79.
Nuffield Council on Bioethics (2007).
Public heath: ethical issues
.
http://nuffieldbioethics.org/wp-content/uploads/2014/07/Public-health-ethical-issues.pdf
Oliver A (2011). Is nudge an effective public health strategy to tackle obesity? Yes.
British Medical Journal
, 342: d2168. doi:
10.1136/bmj.d2168
Panjwani C, Caraher M (2014). The Public Health Responsibility Deal: brokering a deal for public health, but on whose terms?
Health Policy
, 114 (2): 163-73. doi: 10.1016/j.healthpol.2013.11.002
Petticrew M, Eastmure E, Mays N, et al (2013). The Public Health Responsibility Deal: how should such a complex public health
policy be evaluated?
Journal of Public Health
(Oxf), 35: 495-501.
Telfer E (1996).
Food for Thought: Philosophy and Food
. London: Routledge.
Thaler RH, Sunstein CR (2008).
Nudge: Improving Decisions about Health, Wealth, and Happiness
. New Haven / London: Yale
University Press.
CASE 11: England
121
Public health and the food and drinks industry: The governance and ethics of interaction CASE 12: EPODE
Summary
The EPODE International Network is the world’s largest network of childhood
obesity prevention programmes, with 47 dierent EPODE programmes
in 29 countries. (EPODE stands for Ensemble Prévenons l’Obésité Des
Enfants / Together Let’s Prevent Childhood Obesity.) EPODE is a large-scale,
coordinated, capacity-building methodology for communities to implement
eective and sustainable strategies to address the obesity challenge through
interventions aimed at families at the community level. The EPODE methodology
comprises four components: political commitment, public-private partnerships,
community-based actions, and evaluation.
An EPODE programme typically needs 18 months to establish itself and engage
community partners, and three to ve years before its impact is felt. Long-term
sources of programme funding are therefore needed and are a driver of public-
private partnership activity.
Advocates of obesity prevention may oppose public-private partnerships for
both their potential and perceived ethical conicts including: the perception
that the programme will avoid actions that may be in conict with the industry
partner; the potential for the programme to be used as a platform for product
or brand promotion; and the risk of industry inuencing the scientic agenda
and the design of interventions. However, EPODE’s multi-stakeholder approach
promoted through the EPODE methodology has shown encouraging results in
preventing childhood obesity and reducing the socioeconomic gap in obesity.
The role of public-private partnerships in
childhood obesity prevention programmes,
based on the EPODE experience
12
CASE
Authors
Dennis Edell
Director, EPODE
International Network
Jean-Michel Borys
Founder, EPODE
International Network
Pauline Harper
Director Global
Development, EPODE
International Network
Corresponding author
Dennis Edell
Email: dennis.edell@
epodeintergbgnational.
com

122
Public health and the food and drinks industry: The governance and ethics of interactionCASE 12: EPODE
Introduction
Public-private partnership (PPP) can be an important strategy to support health
promotion. The food and beverage industry often emerges as the most interested
private partner for an obesity prevention programme, but these kinds of industry
partnerships may be the most controversial. In this case study we explore how the
EPODE International Network (EIN), the world’s largest network of childhood obesity
prevention programmes, has approached this subject, and some thoughts on our
experience and issues at dierent programme levels.
Obesity is a global epidemic. It is estimated that almost half of the world’s adults will
be overweight or obese by 2030 (Kelly et al, 2008). Childhood obesity is a precursor
to adult obesity – 75% of obese children will become obese adults. It is therefore
important to reverse trends towards obesity through interventions aimed at families
at the community level. EPODE – Ensemble Prévenons l’Obésité Des Enfants /
Together Let’s Prevent Childhood Obesity – is a large-scale, coordinated, capacity-
building methodology for communities to implement eective and sustainable
strategies to address this challenge (Borys et al, 2013).
The EPODE methodology comprises four critical components: political commitment,
public-private partnerships, community-based actions, and evaluation. In large-
scale evaluations, the multi-stakeholder approach promoted through the EPODE
methodology has shown encouraging results in preventing childhood obesity and
reducing the socioeconomic gap in obesity prevalence (Vinck et al, 2016).
Reductions in the prevalence of obese and overweight children in the range of
10% to 20% over three to ve years (Vinck et al, 2016) have inspired a number
of jurisdictions and existing community-based programmes to adopt the EPODE
methodology in order to upscale their eorts to prevent childhood obesity. These
‘EPODE-inspired’ programmes are now the members of the EPODE International
Network. Today there are more than 47 dierent EPODE programmes in 29 countries,
making EIN the world’s largest network of childhood obesity prevention programmes.
The history and organisation of EPODE programmes
EPODE began in 1992 in two small towns in northern France via the vision of a local
health care provider, Dr Jean-Michel Borys. Since that time, multi-year evaluations
of health impacts point to the importance of programme sustainability. Meaningful
health impacts require time to gather actors in the community and to change
social norms in order to inuence the adoption of healthier lifestyles. Typically, a
programme needs 18 months to establish itself and engage community partners,
and three to ve years before its impact is felt and can be measured.

123
Public health and the food and drinks industry: The governance and ethics of interaction CASE 12: EPODE
Many EPODE-inspired community-based programmes are members of a network
of such programmes supported by a ‘backbone’ organisation. The backbone
advocates for the methodology and oers high-level services to community-based
programmes such as training, coaching and knowledge transfer via regional forums.
Protéines, a Paris-based for-prot communications agency, was the rst to serve as
the backbone for a broader network of EPODE-inspired programmes.
Protéines specialises in helping clients to communicate messages to various
audiences about nutritional aspects of their products. Protéines clients have
included major food industry brands such as Ferraro, Danone, McDonald’s, Coca-
Cola and Nestlé. Dr Borys, founder of the EPODE methodology, joined Protéines for
the purposes of leveraging Protéines’ communications services, business acumen
and their client support, to fund the growth of an EPODE network. Protéines was
able to oer its food industry partners a corporate social responsibility vehicle
to be associated with an action to prevent childhood obesity. As the network of
community-based programmes grew, funding for more extensive research projects
was sought from public entities such as the European Commission and the World
Health Organization. However, as a for-prot company, Protéines did not qualify
for these publicly sponsored projects. In April 2011, Protéines formed the EPODE
International Network as an arm’s-length non-governmental organisation (NGO) that
could more easily qualify for large-scale research projects designed to validate the
methodology.
EIN was governed by an independent board (including Dr Borys), but contracted
administrative support and other services from Protéines. By putting the EIN in
place, Protéines maintained the continuity of EPODE and set the stage for the
growth of EIN as an independent and global NGO.
While the relationship with Protéines was symbiotic and positive, EIN found it could
provide, at a much lower cost, the services supplied by Protéines. With the goal of
operating more eciently and resolving any perceived conicts, EIN terminated its
services contract with Protéines in January 2016. Simultaneously Dr Borys ended
his employment agreement with Protéines. In January 2017, EIN’s board decided to
drop its last food industry sponsor. Today EIN operates as a separate entity with no
formal relationship to Protéines.
The sustainability imperative
While mature EPODE programmes can be run eciently, there are costs involved in
hiring local project managers, putting in place a central coordination team, designing
and introducing interventions, and implementing a viable programme evaluation.

124
Public health and the food and drinks industry: The governance and ethics of interactionCASE 12: EPODE
Often the cost of evaluation can equal the cost of running the programme itself.
Long-term, committed and varied sources of programme-funding and programme
champions have therefore been agged as a core issue for sustaining EPODE
programmes and as the driver of public-private partnership activity.
Public-private partnership for funding community-based programmes
Issues relating to funding are well recognised in the health intervention literature
(Jacobs et al, 2012) and hence the salience of public-private partnership is not
surprising. However, the diering nancial support environments of the various
programmes, and the varying ability to establish consistent guidelines for procuring
and maintaining funding, highlight the diculty of navigating this issue in multi-
country collaborations.
In the 25 years since the EPODE programme was rst eld-tested, varying public-
private partnership schemes have been tried and now exist at three levels:
1 Support for the ‘backbone’ or EIN level – for example, the organisation that
supports community-based programmes and provides scientic advice and
operational training.
2 Support for programme management – the central coordination team at the
national, state or provincial level.
3 Support at the local community level for activities initiated by the local project
manager.
In terms of sources of funding, EPODE programmes vary on the continuum of
receiving 100% public funding to 100% private-sector funding, with 65% to 75%
of EIN programme members having some combination of both private and public
funding.
The food and beverage industry has been the rst to step up and oer assistance
to EIN and EPODE programmes. This is not surprising given the amount of criticism
they receive for the role of the industry as contributors to the problem of obesity.
The food and beverage industry is anxious to defend its reputation and many
industry members genuinely want to nd a way to be part of the solution. Some
have done so by oering healthier product choices or by supporting programmes
aimed at reducing the prevalence of obesity, such as EIN. For industry partners
hoping to build trust among consumers and political authorities, PPPs are important
for corporate social responsibility and public relations (Borys et al, 2012). PPP
relationships between a food or beverage industry partner and an NGO like EIN
provide a platform from which a corporation can declare to socially responsible

125
Public health and the food and drinks industry: The governance and ethics of interaction CASE 12: EPODE
investors a concern for the health of children and point to their support of EIN as a
tangible expression of this concern.
Funding from the food and beverage industry may help to guarantee sustainability
and therefore encourage measurable positive health impacts from a community-
based childhood obesity prevention programme. However, many advocates of
obesity prevention still oppose this kind of PPP for both its potential and perceived
ethical conicts. These concerns need to be recognised and addressed and include
the following:
• The perception that the programme will avoid actions that may be in conict with
the industry partner. For example, programmes under industry pressure might
choose not to advocate for disincentives such as taxation of sugar-sweetened
beverages to encourage greater water consumption.
• The potential for the programme to be used as a platform for product or brand
promotion through branding, visibility of marketing actions, or product sampling
(no matter how healthy the product may appear to be). An overt example is
Nestlé’s Healthy Kids, a corporate-branded programme promoting healthy
lifestyles that is 100% funded by Nestlé.
• Inuencing the scientic agenda and the design of interventions, in order to avoid
conict with an industry action or business goal. Examples of possible conicts
include:
– Industry may prefer to focus messages on balanced energy intake (calories),
when the issue is the high sugar content of the product.
– Industry may not support promoting drinking water if the programme excludes
the purchase of bottled water as an option.
– Industry may resist any attempt to call attention to, or limit the marketing of,
unhealthy foods to children.
In its approach to PPP, EPODE has anticipated and attempted to address these
ethical issues to create a framework where PPP can work to the benet of the
children and to improve the impact of the programme on reducing the number
of obese and overweight children. This has worked in some cases and may be
instructive for programmes considering this form of PPP.

126
Public health and the food and drinks industry: The governance and ethics of interaction
Case
EPODE’s experience and its process for managing these private-partner
relationships have shown that an enlightened private industry partner can contribute
in a positive manner without conicts. In theory, a healthy and frank dialogue with
food and beverage companies should benet both parties to the partnership.
If a private partner is involved in an EPODE programme, the relationship is governed
by a long-term Commitment Charter that guarantees mutual respect and trust for
each party (Borys et al, 2015). Private partners must accept and commit to the
following conditions:
1 Never associate the programme with their products.
2 Never inuence the content of the programme.
3 Only communicate on the programme in internal or corporate communications.
Even when a Commitment Charter is in place, often it may not be enough to prevent
criticism. Critics feel that accepting funding from the food and beverage industry
detracts from the appearance of legitimacy, independence, and eectiveness of the
EPODE approach. This perception of bias may make it dicult to engage potential
and current non-industry funders and other stakeholders (Pettigrew et al, 2014).
Academics in particular fear that PPP funding will raise questions about the
legitimacy of their scientic agenda. They have been vocal in their objections to
EIN relationships with food and beverage partners, and some have disavowed any
relationship with EIN because of its advocacy of PPP.
Public health practitioners and some non-governmental organisations have also
voiced suspicion about the motives of food and beverage corporations. They see
industry support for EPODE programmes as a thinly veiled attempt to mollify critics
and allow them to continue to market unhealthy products.
This criticism of industry is not unfounded. The food and beverage industry
struggles with the contradiction of a desire to be responsive to the health needs
of their customers while at the same time being robust marketers of products
of questionable health properties. Recently, in the 2017 Report on the Health
of Canadians by Heart and Stroke, food and beverage marketers were strongly
criticised for marketing unhealthy food to children. In 2015, it was discovered
that Coca-Cola was the primary funder of a new scientic organisation promoting
balanced energy intake, an argument the beverage industry uses to divert attention
away from sugar content. And when public agencies enact or threaten to enact
consumption taxes on some foods or sugar-sweetened beverages, the industry may
CASE 12: EPODE
127
Public health and the food and drinks industry: The governance and ethics of interaction
employ aggressive marketing tactics to vigorously oppose taxation (Kmietowicz,
2015; Pollan, 2016; Heart and Stroke, 2017).
These controversies are not one-sided. The perception of risk can also be an
obstacle to participation by food and beverage industry partners. They fear that
they can never satisfy their critics’ desire for reformulation, nutritional labelling or
elimination of products without unduly compromising their business model. In a time
of transparency and increased public pressure for accountability, some major players
in the food and beverage industry have become cautious about publicly supporting
obesity prevention. Declining sales of sugar-sweetened products have put some
companies under pressure to nd new sources of revenue. Companies have been
publicly called out for inuencing scientic research (Bes-Rastrollo et al, 2013).
And the public debate around legislative options such as a ‘sugar tax’ to curtail
consumption puts companies in a situation of conict. Public support for obesity
prevention by beverage companies may be perceived as them ‘buying’ their way out
of taxation.
Based on the EPODE experience, these concerns are not shared across all forms
of PPP or at all programme levels, but can be seen as a continuum of concern, as
shown in Figure 1.
In the vertical axis, concern about PPP occurs mostly at the higher level of
programme coordination rather than in local actions. For example, at the lower level,
local EPODE project managers routinely create partnerships with food stores and
quick-serve restaurants to promote programme awareness, or for in-store nutrition
Food and beverage
industry partners
Figure 1: Concern about public-private partnerships
Central
Local
Source of funding
Concern
Level of funding
Non-food and
beverage partners,
e.g. bank,
insurance company
CASE 12: EPODE

128
Public health and the food and drinks industry: The governance and ethics of interactionCASE 12: EPODE
education activities conducted inside the stores themselves, such as school trips to
the local market produce section to learn about fruits and vegetables or discover
new fresh food ideas.
However, at the higher programme coordination level, there are more concerns
about private partnership and the inuence of industry. Public funders – as in the
case with OPAL (Australia) or Healthy Kids Community Challenge (Canada) – may
avoid any funding partnerships with industry for fear that their programmes may
be compromised by the appearance and perception that industry is inuencing
programme design or in some way proting from an association with government.
Other EPODE-inspired programmes, such as JOGG in the Netherlands, have no
hard and fast rule but review partnerships on a brand-by-brand basis.
On the horizontal axis, concern grows with the identity of the funder and the
ensuing sense of a perceived conict of interest and objections from stakeholders.
Partnerships with a processed food company or a sugar-sweetened beverage brand
are at best an uneasy alliance for the reasons detailed above, while private partners
that are not associated with food or beverage brands – such as banks or insurance
companies – do not appear to be in conict. In fact, within the obesity sphere
even partnerships with pharmaceutical companies, that often elicit caution from
researchers, have not suered the same degree of stigma as those with large food
and beverage brands such as Coca-Cola, PepsiCo or McDonald’s.
Alternative scenarios
The wisdom of the involvement of the food and beverage industry with childhood
obesity prevention programmes continues to be debated by the board of EIN. Food
and beverage manufacturers are under public pressure to oer healthy choices
and also face legislative action, and so have an incentive to be seen to be helping
to solve the problem of childhood obesity. They will continue to have an interest in
supporting viable programmes and science-based methodologies such as EPODE
that have proved successful in addressing the problem of childhood obesity.
While the Commitment Charter works in most cases, other options are open to
programme managers. Some of the following options have been considered and in
some cases put into operation.
1
Reject PPP
: We may decide that there may be no way to resolve the appearance
of a conict when accepting support from food and beverage companies. The
choice is either to carry on and accept the criticism, or drop all partnerships with
food and beverage manufacturers and seek less controversial sources of PPP
funding.
129
Public health and the food and drinks industry: The governance and ethics of interaction
2
Alternative structure
: Some jurisdictions (e.g. Aruba, Chile) opted to create
healthy community foundations that are separate from, but may have a close
relationship with, government. Foundations are seen to be at arm’s length from the
government and are therefore able to manage population-based programmes and
accept donations from both public and private sources.
3
Industry changes
: Manufacturers of food and beverage products claim they full
a consumer need for processed or sweetened foods based on consumer wants.
Could they be more accepting of a fundamental shift in their business model?
This would require placing limits on selling unhealthy products and in formulating
and promoting healthy products even if they are contrary to current consumption
habits, and requires changing the perception of desirable taste – for example, less
sweet or salty becoming more acceptable.
Discussion
Case questions
1 Are dynamic, positive relationships with food industry partners possible without fatally
damaging the credibility of the programme?
2 Does the reward of a sustainable programme outweigh the risk from receiving funding
from food and beverage industry sources?
3 Is there a hierarchy of perceived conflicts when considering food and beverage industry
partners: brands or subsectors that would lead to exceptions?
4 Is the perception of conflict too great to overcome, even with safeguards like a
Commitment Charter in place?
5 Given that it is difficult to ‘prove’ that private partners do not interfere with programmes,
what indicators can be used to ensure transparency?
6 Under what conditions would industry be willing to make tangible commitments to make
changes to their business model – for example, selling less unhealthy products and
promoting healthier products – even if these were not consistent with current consumer
tastes? Would the threat of legislation (consumption tax) help persuade them?
There is general agreement that some form of PPP is needed for sustainable
funding, and with the idea that the food and beverage industry must be involved
in solving the problem of high rates of obese and overweight children. However,
the inability to gain widespread acceptance of PPP among stakeholders has made
these partnerships problematic.
CASE 12: EPODE

130
Public health and the food and drinks industry: The governance and ethics of interaction
Public funding free of industry is not the answer. We need varied sources of funding.
We have seen large-scale government-sponsored programmes lose their funding for
no reason other than a dierent political party coming to power.
Any discussion of PPP and the relationship with the food and beverage industry
should consider both practical and ethical issues. In practice, a meaningful reduction
in the prevalence of obesity requires long-term support, which EPODE has shown
requires a mix of both public and private funding.
The most promising source of this funding is often food and beverage companies
that feel a responsibility to step up and be part of the solution. As food and
nutritional choices are fundamental to obesity prevention, it seems counter-
productive not to include the food and beverage industry in the discussion and as
partners in nding the solution.
On the other hand, industry should be given credit when oering healthier products
and for making improvements in recipes that have reduced sugar, salt and fat. They
have put forward several public-facing solutions – such as reduced portion size,
healthier line extensions, and more transparent labelling – but they still have a long
way to go. For the most part they have avoided fundamental and costly systemic
changes such as eliminating agship product lines, or reformulations that require
reorienting consumers’ tastes.
Hopefully we can come to a common ground between public health concerns
and the actions of food and beverage manufacturers. We have seen how public
awareness of the magnitude of obesity levels can result in changes in consumption
patterns. For example, more water is now being consumed, with a corresponding
signicant decline in sales of SSBs.
As we have discussed, public-private partnership with the food and beverage
industry is happening and good partnerships are possible. Industry feels the public
pressure, and has already made small changes in portions and formulation. And
they have sought to associate themselves with solutions and accept partnerships
with restrictions on brand promotion and visibility as per the EPODE Commitment
Charter. Under these scenarios it may be possible for PPP to be more acceptable to
both parties and to lead to a solution where PPP can be a signicant contributor to a
reduction in levels of childhood obesity.
CASE 12: EPODE
131
Public health and the food and drinks industry: The governance and ethics of interaction
Declarations of interests
Dennis Edell
None declared.
Jean-Michel Borys
Jean-Michel Borys held an honorary, non-executive role as Vice President of Protéines, a professional communications company
specialising in the food sector, until 2016.
Pauline Harper
Processed food and beverage industry:
• In 2015 EPODE International Network (EIN) received €45,000 from the Coca-Cola Company and €300,000 from Nestlé SAS.
• In 2016 EIN received CHF 100 000 / €90,000 from Nestlé SAS.
• From September 2016 to February 2017 my company a2bc received remuneration from the Consumer Goods Forum for me to
cover a maternity leave as Interim Director of Health and Wellness.
Marketing, advertising or PR
: I was a salaried employee of Protéines Communication Agency, Paris, France, until the end of
December 2015.
References
Bes-Rastrollo M, Schulze MB, Ruiz-Canela M, Martinez-Gonzalez MA (2013). Financial conicts of interest and reporting bias
regarding the association between sugar-sweetened beverages and weight gain: a systematic review of systematic reviews.
PLOS
Medicine
. https://doi.org/10.1371/journal.pmed.1001578
Borys J-M, Le Bodo Y, Jebb SA, et al (2012) EPODE approach for childhood obesity prevention: methods, progress and internation-
al development.
Obesity Reviews
, 13 (4): 299-315. https://www.ncbi.nlm.nih.gov/pmc/articles/PMC3492853/
Borys J-M, Valdeyron L, Levy E, et al (2013). Obesity and weight management. EPODE – A model for reducing the incidence of
obesity and weight-related comorbidities.
US Endocrinology
, 9 (1): 32-36. http://doi.org/10.17925/USE.2013.09.01.32
Borys J-M, Graça P, Gregorio MJ, et al (2015).
EPODE for the Promotion of Health Equity
. Cachan, France: Lavoisier Publishing.
http://epodeinternationalnetwork.com/wp-content/uploads/2016/03/EPHE_BOOK.pdf
Heart and Stroke (2017).
The Kids are Not Alright. How the Food and Beverage Industry is Marketing our Children and Youth to
Death. 2017 Report on the Health of Canadians
.
http://www.heartandstroke.ca/-/media/pdf-les/canada/2017-heart-month/heartandstroke-reportonhealth2017.ashx
Jacobs JA, Jones E, Glabella BA, et al (2012). Tools for implementing an evidence-based approach in public health practice.
Preventing Chronic Disease
, 9: 110324. http://dx.doi.org/10.5888/pcd9.110324
Kelly T, Yang W, Chen CS, et al (2008). Global burden of obesity in 2005 and projections to 2030.
International Journal of Obesity
(Lond)
, 32: 1431-37. https://www.nature.com/articles/ijo2008102
Kmietowicz Z (2015). Coca-Cola funded group set up to promote ‘energy balance’ is disbanded.
British Medical Journal
, 351:
h6590. https://doi.org/10.1136/bmj.h6590
Pettigrew S, Borys JM, Ruault du Plessis H, et al (2014). Process evaluation outcomes from a global child obesity prevention
intervention.
BMC Public Health
, 14: 757. doi: 10.1186/1471-2458-14-757
Pollan M (2016). Big Food strikes back. Why did the Obamas fail to take on corporate agriculture?
New York Times Magazine
, 5
October 2016. http://www.nytimes.com/interactive/2016/10/09/magazine/obama-administration-big-food-policy.html?_r=0
Vinck J, Brohet C, Roillet M, et al (2016). Downward trends in the prevalence of childhood overweight in two pilot towns taking
part in the VIASANO community-based programmes in Belgium: data from a national school health monitoring system.
Pediatric
Obesity
, 11 (1): 61-67. doi: 10.1111/ijpo.12022
CASE 12: EPODE

132
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 1
Authors
Alafia Samuels
Director, George
Alleyne Chronic
Disease Research
Centre, University
of the West Indies,
Barbados
Maisha Hutton
Executive Director,
Healthy Caribbean
Coalition
Trevor Hassell
President, Healthy
Caribbean Coalition
The timely collection of cases in this Casebook illustrates the continuing challenges
of managing competing public and private interests in implementing nutrition and
alcohol policy in diverse settings. Many Caribbean countries are exploring scal
policies to reduce obesity, in particular reducing consumption of sugar-sweetened
beverages (SSBs). Eleven of the 15 countries with the highest obesity rates in the
world are small-island developing states of the Pacic and the Caribbean, which lack
food sovereignty and are highly dependent on imported foods. The case studies
raise the important issue of dening and limiting the role of industry in the interest of
safeguarding nutrition-related policy and legislation.
In 2015, Barbados became the rst Caribbean country to impose a tax on SSBs
aimed at slowing and reversing the epidemic of obesity and overweight and its
sequelae, in a country which has high SSB consumption, and in which NCDs result
in 75% of premature deaths (30-69 years) – double the rate in North America – and
which account for more than 60% of the health budget.
The announcement of Barbados’ intention to enact legislation to tax SSBs was
met by a response from the SSB industry very similar to that experienced by
many countries featured in this Casebook. This took the form of initial support for
appropriate public health policies. However, once it was recognised that one of
the policies would be the enactment of legislation to impose a tax on SSBs, robust
opposition ensued, including the recommendation of physical activity as an alternate
and eective option, the oer of nancial support for implementation of nationwide
physical activity programmes, and the advancement of industry-provided research
to show the ineectiveness of imposing taxes to reduce overweight and obesity.
The resistance of the SSB industry to the imposition of the tax was made in mostly
undocumented meetings between the political leadership of Barbados and leaders
and lobbyists of major international SSB producers. It was undertaken in this manner
due to the absence of a requirement at national level that interactions between the
public and private sectors for the prevention of NCDs be made known to the general
public. Subsequently, recognising this deciency, the Healthy Caribbean Coalition
(HCC) and the University of the West Indies (UWI) produced case studies and briefs
which documented the process that led to the tax on SSBs and the subsequent
response by a global leader of the SSB industry.
National NCD Commissions – multi-sectoral platforms established in Barbados
and throughout the Caribbean as outcomes of the 2007 Port of Spain Heads of
Government Summit on NCDs – have the potential to be mechanisms to document
interactions between the public and private sectors on NCD prevention and
control. However, this platform and others including national social partnerships of
Commentary 1 –
A perspective from the Caribbean
COMMENTARY
1

133
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 1
government, private sector and trade unions, have not been eective in addressing
the challenges of NCD prevention and control.
The experience of the Fiji Ministry of Health-led ‘public-private initiatives’ (PPI) with
the food industry (Case 3) illustrates the importance of dening rules of engagement
and delineating clear boundaries with the food and beverage sector. Early in 2017
in Jamaica, a similar approach to the Fiji PPI was used with the formation of a
National Food Industry Task Force (NFITF), with multi-sectoral, broadly inclusive
representation, including a signicant private sector presence (in contrast to Brazil’s
‘collective’ which excludes the private sector). The NFITF is primarily tasked with
advising the Minister of Health on nutrition policy and legislation. The ecacy of
this task force as a transparent mechanism for catalysing measurable industry
action (whether through policy recommendation or voluntary self-regulation – one
beverage company has already ‘pledged’ to reduce sugar content in its products by
30%) remains to be seen, including the extent to which ethical issues arise and are
managed. There may be some value to this approach in small nation states, where
personal and professional relationships intersect heavily. However, this was not the
experience in Fiji and the case studies presented here demonstrate that industry has
a familiar playbook of deceptive tactics and rarely prioritises public health interests
above its own. Civil society organisations, such as the Heart Foundation of Jamaica,
will need to leverage past experience with the tobacco industry to anticipate and
rebut old industry tactics. The National NCD Commission in Jamaica may serve as a
vehicle through which conict of interest (COI) policies can be developed to govern
private sector relationships in the NFITF.
The relationship with the alcohol industry is even more nuanced and fraught with
considerable political and economic challenges which raise a myriad of complex
conict of interest issues not easily addressed in our economically vulnerable small-
island settings.
The challenges posed in the Caribbean by public-private interactions for the
prevention and control of NCDs are often occasioned by an apparent unawareness
of the potential for conict of interest, a general lack of appreciation of the potential
for the private sector to frustrate the eorts of the public sector in NCD prevention,
and the strong economic inuence of the private sector on the small nation states
of the Caribbean. Practitioners, policy-makers and civil society need competencies
and skills including in advocacy, accountability, management of conict of interest,
and increasing public education and awareness in an eort to navigate public-private
interactions in the Caribbean as part of the multi-sectoral response to NCDs.
134
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 1
Many of the challenges highlighted have been recognised and form the strategic
pillars of the Healthy Caribbean Coalition Strategic Plan 2017-2021 and have been
actioned by the Healthy Caribbean Coalition using varied approaches including the
hosting of workshops, production of policy briefs, interaction with policy-makers,
and capacity-building of civil society organisations. HCC and other key regional
players – such as CARICOM (the Caribbean Community), Pan American Health
Organization / WHO, the Caribbean Public Health Agency and University of the West
Indies – in responding to the call for NCD multi-sectorality, are increasingly aware of
potential ethical landmines that exist when engaging the private sector. However,
the challenge arises with managing global guidance around conict of interest and
the economic and cultural realities of small-island developing states. More needs to
be done by regional and global public health agencies and national governments in
providing direction, guidance, technical assistance, policies and programmes that
recognise country and regional contexts while reecting international best practice in
the multi-sectoral approach to NCD prevention and control, especially as this relates
to the participation of the food and beverage industries.
Declarations of interests
Alafia Samuels
None declared.
Maisha Hutton
Financial services
: Insurance/banking: The Healthy Caribbean Coalition (HCC) is funded primarily by the Life Insurance Industry,
Sagloor Life Inc, Barbados. The HCC has also recently signed an MOU with a major regional banking firm – CIBC/FCIB (First
Caribbean International Bank).
Trevor Hassell
Financial services
: I have an advisory role in insurance industry in Barbados.

135
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 2
Authors
Paula Johns
Executive Director,
ACT Health
Promotion, Brazil
Ana Paula Bortoletto
Leader of the
Healthy Diets
Program, Instituto
Brasileiro de Defesa
do Consumidor
(Brazilian Institute of
Consumer Protection)
A background of changing political trends in several countries in the Americas
towards a more pro-business mindset, and the economic crisis, have been leading
to the tempting and simplied solution of seeing the market as the natural solution
for our common social challenges. This in turn has led to an increased willingness
to privatise services in all areas (including health) and to invest in public-private
partnerships (PPPs) as the ultimate solution. In this scenario, it is extremely relevant
to reect upon, understand and identify the impact of those partnerships in public
health outcomes, both in the regional and national contexts.
The case studies collected in this Casebook bring to light important aspects that
contribute to that debate. Case 3 about Fiji and Case 11 about the Public Health
Responsibility Deal in England are two examples that show the limitations and failure
of PPPs to achieve public health goals. The conclusion could be that, besides
not contributing to its stated objectives, the PPP also serves as a diversion from
focusing on other potentially more eective measures. In Cases 2 and 6 from
Chile we can see two other important dimensions: rstly, about how the economic
players of a given government tend to be more powerful than the health players;
and secondly about how this has consequences in undermining the independence
and autonomy of research in universities. Another theme that arises from more than
one case study is governance and how this has a direct impact on public health
outcomes – for example, when civil society does not have established mechanisms
for participation.
Case 10 about the Global Health Council and the UN High-level Meeting on Non-
communicable Diseases (NCDs) raises an excellent discussion about how PPPs in
the area of NCDs tend to benet the private more than the public interest. It also
sheds light on the need to have more transparency and not to put all civil society
stakeholders in the same category, as it makes it harder to dierentiate between
organisations representing public interests and those representing commercial
interests. Many of the case studies conrm the evidence that shows that self-
regulation is not eective in achieving public health goals, and that voluntary
agreements with industries that are causing the problem provide a platform that
allows for even greater industry inuence in policy-making processes.
Case 12 about EPODE brings a more positive view on PPPs, and is useful at
dierentiating the situations of PPPs in dierent settings. However, it does not
include an evaluation of the impact of the initiative and seems to focus more on
the methodology and the partnership for its own sake. It also fails to recognise
the problem with partnerships with multi-national corporations that have dierent
practices depending on the situation of the context. For example, how can you
guarantee that a food company is a trusted legitimate partner in a small city in
Commentary 2 –
A perspective from the Americas
COMMENTARY
2

136
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 2
France while it still markets breastfeeding substitutes directly to mothers in a small
city in São Paulo? Can it really be described as an ‘enlightened industry partner’, or
is it just defending its business interests as best it can?
The understanding about conicts of interest and its impact on the design of
public policies is still limited in the Americas and in global health governance, as
shown by the many references in the case studies. We do not have a systematic
way of documenting corporate political activity, as most of the practices are not
as transparent as they should be and there is no policy coherence from one place
to another or within dierent government branches. For example, of the dozens
of public relations companies operating in Brasília, hired by large corporations to
monitor the policy-making process that can impact their commercial interests, none
discloses who their clients are in their public websites, nor presents themselves as
having been commissioned by those companies.
The best positive example of documenting public-private interactions for the
prevention of NCDs is the case of tobacco control, in which the tobacco industry
stakeholders have been explicitly framed as the cause of the tobacco epidemic in
a legally binding international health treaty (the WHO Framework Convention on
Tobacco Control). Several measures have therefore been taken to mitigate the risk
of undue interference in policy-making processes, although not necessarily making it
easier to implement this in practical terms.
Even within the WHO structure, the stricter treatment given to the tobacco industry,
thanks to the Framework Convention on Tobacco Control, is not automatically
translated into practice for other risk factors in which the policies, practices and
impact of a particular product on public health do not dier from the tobacco
example. The presence of the alcohol industry and ultra-processed products
industries in the decision-making processes is still signicant.
The political process – at national, regional and international level – is captured by
the economics of private corporate interests. The reasons why private corporate
interests are having undue inuence, and why we are having diculty guaranteeing
public interest in complex societies, include: campaign funding for politicians;
revolving doors between regulatory agencies and the to-be-regulated corporate
sector; media campaigns; and funding of research. An important factor that
underpins all of the above reasons is that we have created rules for the operation
of markets that allow for-prots with no limits and ignore (or fail to account for) the
social and environmental externalities in the most protable sectors of business.
137
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 2
To deal properly with conicts of interest, we rst need to give the issue the attention
it deserves. We need to develop critical mass to interpret the world beyond the tip of
the iceberg. We need to have established mechanisms for civil society participation,
dierentiating public from private interests. We also need to have a clearer denition
– which in the area of nutrition could be fairly simple – of which particular parts of
the private sector we want to guarantee a seat for at the negotiation table. In that
sense, it is crucial to dierentiate small producers of healthy, natural, minimally
processed or processed products from the manufacturers of ultra-processed food
and drink products that should not even be classied as real food. The latter should
not have a seat at the table. We need a framework to analyse those elements, and
a useful approach is the one presented by Mialon et al in ‘A proposed approach to
systematically identify and monitor the corporate political activity of the food industry
with respect to public health using publicly available information’ (Mialon et al, 2015).
There are several small initiatives, led by public interest civil society organisations,
aimed at exposing industry practices in order to move forward with regulatory
policies. Civil society needs to play the role of watchdog, examining what is
happening in these interactions and their impact. It would be excellent for global
public health governance to move beyond the multi-sectoral approach as the
predominant mantra for NCD prevention and control, and to create eective
monitoring and screening methodologies to expose corporate political activities that
are taking place on a daily basis all over the world against eective measures to
tackle the burden of malnutrition in all its forms, and to help markets that support
producers of healthy fresh foods and grains free from pesticides and antibiotics.
Why does the world still accept that ultra-processed product companies still target
children in their unethical marketing strategies? Why does the world still accept false
and misleading labels on consumer products? Why is it more protable to produce
superuous and harmful sugary drinks than to survive as a farmer who produces
healthy and nutritious fresh foods?
Declarations of interests
Paula Johns
Pharmaceutical: A grant from Medtronic was processed through the NCD Alliance.
Ana Paula Bortoletto
None declared.
References
Mialon M, Swinburn B, Sacks G (2015). A proposed approach to systematically identify and monitor the corporate political activity
of the food industry with respect to public health using publicly available information.
Obesity Reviews
, 16 (7): 519-30. doi:
10.1111/obr.12289. Epub 19 May 2015.

138
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 3
Author
Katrin Engelhardt
Technical Lead,
Nutrition, WHO
Western Pacific
Region (at the time
of writing)
The double burden of malnutrition – where overnutrition increasingly occurs
alongside undernutrition in developing countries – is fuelling the complexity of
engagement with non-state actors. The case studies in this Casebook highlight
challenges that arise when engaging with for-prot entities that produce unhealthy
foods, or with industry-funded ‘front groups’. The case studies suggest elements
that are critical to safeguarding public health from vested interests. These are very
relevant to the Western Pacic region, a region where progress has been made
on reducing chronic undernutrition (stunting) in some countries, while childhood
overweight is increasing, and overweight among adolescents aged 13-15 years is as
high as 60% in some countries.
The WHO Commission on Ending Childhood Obesity has recommended countries
“to develop guidelines, or policy measures that appropriately engage relevant
sectors – including the private sector, where applicable – to implement actions,
aimed at reducing childhood obesity” (World Health Organization, 2016). However,
recognising the potential risk of engagement, the draft implementation guide on
Ending Childhood Obesity (World Health Organization, 2017) proposes as a rst
step that countries should “establish mechanisms to coordinate the engagement of
non-state actors and hold them to account in the implementation of interventions”
and to “establish clear mechanisms / policies for the management of conicts of
interest.”
The importance of this is apparent in most of the case studies, including those from
Chile, Guatemala and Brazil (Cases 2, 4, 6 and 8). Case 3 from Fiji shows that, if
such mechanisms are not in place, eorts by the Ministry of Health to implement
policies to promote healthy diets and create healthy food environments are easily
undermined by the food industry. Virtually none of the countries in the WHO Western
Pacic region have explicit commitments or measures to prevent and manage
conicts of interest in their national nutrition-related policies (unpublished review).
Before engaging with any non-state actor, Ministries of Health are encouraged to
conduct due diligence on the potential partner (i.e. gather information about the
non-state actor), and as a second step, assess the risk of engagement (focusing
on the type of proposed engagement). It is critical for Ministries of Health, or other
Ministries such as the Ministry of Education, to understand the interests of the
non-state actors before engaging them in public health actions, especially with
for-prot entities with commercial interests and/or their front groups, or with public-
private partnerships through which for-prot entities may engage in and shape food
and nutrition policies (e.g. as described in Case 10 on the Global Health Council
or Case 12 on EPODE). Gomes proposed reviewing the products, practices and
Commentary 3 –
A perspective from the Western Pacific region
COMMENTARY
3

139
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 3
policies of for-prot entities to better understand their interests (Gomes, 2015). For
example, if a for-prot entity produces a product which is not in line with national
dietary recommendations (e.g. breast-milk substitutes, or products high in salt, free
sugars or fats), or if that entity markets these products to children using deceptive
or persuasive tactics, then this entity’s interests are likely to oppose the interest of
the Ministry of Health or the Ministry of Education that is attempting to create healthy
food environments, for example for school children.
Reecting on the situation in the Western Pacic region, country eorts to improve
nutrition and healthy diets are facing similar challenges to those outlined in the
case studies. Push backs from the food industry have been observed in country
attempts to tax sugar-sweetened beverages, to implement school food standards,
and to restrict food marketing (of breast-milk substitutes, unhealthy foods, and
non-alcoholic beverages). It is common for the food industry to propose voluntary
pledges on food marketing, on front-of-pack labelling of pre-packaged foods, or on
reformulation of foods, as described in the case studies from Fiji, England or Mexico
(Cases 3, 7 and 11). However, the experiences in Fiji and in the UK show that
voluntary approaches did not result in improving the food environment. Evidence
is accumulating in favour of regulatory action to improve nutrition and healthy diets
(Kunkel et al, 2015; Galbraith-Emami and Lobstein, 2013).
Within the Western Pacic region there are several gaps that hinder regulatory
action to create healthy food environments in which the healthy decision is made
the easy decision. Firstly, there may be a lack of civil society organisations and
consumer protection groups to advocate for healthy diets, to raise awareness of
unhealthy diets, and to galvanise public support. Secondly, there may still be a
lack of awareness of interference tactics in policy-making by the food industry and
their front groups, and a lack of awareness about the potential risks of engaging
with non-state actors. To increase awareness about these issues, it is important
to integrate them into the training of health professionals, including in training for
medical doctors, nurses, midwives, dietitians and nutritionists. Thirdly, the region
could benet from expanding its network of public interest lawyers to support policy-
making. The region can learn from the experiences in tobacco control, and be better
prepared to counter interference in the policy development cycle.
It is critical to realise the importance of good nutrition and healthy diets throughout
the life course, starting with exclusive breastfeeding, when food preferences are
shaped. Ministries of Health are encouraged to take a leadership role in creating
healthy food environments, to establish clear mechanisms and policies for the
management of conicts of interest, and to act in the public’s interest.
140
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 3
Declarations of interests
Katrin Engelhardt
None declared.
References
Galbraith-Emami S, Lobstein T (2013). The impact of initiatives to limit the advertising of food and beverage products to children:
a systematic review.
Obesity Reviews
, 14: 960-74.
Gomes F (2015). Conflicts of interest in food and nutrition.
Cadernos de Saúde Pública
, 31: 10.
Kunkel DL, Castonguay JS, Filer CR (2015). Evaluating industry self-regulation of food marketing to children.
American Journal of
Preventive Medicine
: 49 (2): 181-87.
(Unpublished review.) Unpublished review conducted by WHO/WPRO in preparation for the midterm review of the Action Plan to
Reduce the Double Burden of Malnutrition in the Western Pacific Region (2015-2020).
World Health Organization (2016).
WHO Report of the Commission on Ending Childhood Obesity
. Geneva, Switzerland: World
Health Organization.
World Health Organization (2017).
Report of the Commission on Ending Childhood Obesity: implementation plan
.
http://apps.who.int/gb/ebwha/pdf_files/WHA70/A70_31-en.pdf

141
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 4
Authors
Cecile Knai
London School of
Hygiene and Tropical
Medicine
Mark Petticrew
London School of
Hygiene and Tropical
Medicine
This Casebook highlights the fact that well-rehearsed corporate political strategies
(vividly illustrated in Cases 2 and 6 from Chile) are systematically employed by the
industry (and in a highly similar way) to defend the industry’s economic interest.
The case studies presented here highlight the shifting locus of public health policy
governance, partly resulting from a vacuum left by budgetary restrictions in public
health (illustrated in Case 9 from Spain) and from the problematic concept of
‘inclusivity’ (illustrated in Case 10 about the Global Health Council, Case 7 from
Mexico, and Case 3 from Fiji), which seems not to be accompanied by critical
assessment of accountability and conict of interest.
The journey toward self-regulation or voluntary agreements, as demonstrated in
Case 9 from Spain and Case 3 from Fiji, is highly relevant to England, where the
food and alcohol industry were involved in designing and steering a public-private
partnership with the government (the Public Health Responsibility Deal) which has
been evaluated as ineective on the whole (Knai et al, 2017; Knai et al, 2016; Knai et
al, 2015a; 2015b; 2015c; 2015d; Petticrew et al, 2016; Durand et al, 2015).
The Chilean case study on research funding from the food industry (Case 6) also
resonates with experiences in England. We have written about the inherent conict
of interest underpinning a current consortium of food industries and public research
bodies to fund food research, highlighting the unequal nancial contribution of
parties, with the industry never exceeding 10% contribution, all the while driving the
research agenda towards studies which are not likely to be addressing the global
burden of nutrition-related diseases, but rather which will meet the industry’s needs
(Knai et al, 2010).
Key competencies and skills needed for the public health community to eectively
navigate public-private partnerships include far greater literacy in conict of interest
management, as highlighted in Case 9 from Spain, citing Galea and McKee (Galea
and McKee, 2014). A crucial point made in Case 10 about the Global Health
Council is that “aording equal voice to business and other segments of civil society
masks interests”. Moreover Case 9 from Spain underscores the importance of clear
leadership on public health and calls upon relevant government departments to
take on that leadership. Yet, it is essential to acknowledge that the line between the
public sector (government) and the private sector (industry) is often blurred, with
‘revolving doors’ between government and industry. In the case of the Public Health
Responsibility Deal, a public-private partnership with the food, alcohol and other
industries in England with the stated goal of improving health, a former government
operative moved to take on the leadership of an alcohol industry ‘responsibility
body’, the Portman Group. He later led the strand of the Responsibility Deal that
focused on alcohol harm reduction.
Commentary 4 –
A perspective from the UK
COMMENTARY
4

142
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 4
This brings us back to the fact that decision-making in public health is shifting and
increasingly complex and diversied, requiring acknowledgement that the interests
of the ocial ‘public sector’ are not always aligned with those of the public health
community.
Indeed as highlighted in Case 11 on the Public Health Responsibility Deal in
England, the lack of oversight by an arm’s length agency clearly mandated with
public health authority, as well as limited accountability and independent monitoring,
created a situation where industry interests appeared to dominate over public
health objectives, as reported in a series of research papers on the evaluation of
the Responsibility Deal (Knai et al, 2017; Knai et al, 2016; Knai et al, 2015a; 2015b;
2015c; 2015d; Petticrew et al, 2016; Durand et al, 2015).
Overall, these case studies reect the wider literature in concluding that partnerships
and voluntary agreements involving industry aimed specically at improving the
public’s health are not the most eective approach to meet public health objectives
(Downs et al, 2013; Hendry et al, 2015; Jensen and Ronit, 2015; Ronit and Jensen,
2014; Kunkel et al, 2015; Potvin Kent and Wanless, 2014; Potvin Kent et al, 2011;
Noel et al, 2017; Huizinga and Kruse, 2016; Bartlett and Garde, 2015). They reect
that, on the whole, industry motivations for partnerships in public health policy are
predominantly about enhancing reputation, meeting corporate social responsibility
commitments, and ultimately avoiding, weakening and delaying regulation (Durand
et al, 2015).
Researching public-private partnerships
It is also worth noting that researching and evaluating public-private partnerships
can itself be challenging – as one would expect of any evaluation of a complex and
politically sensitive intervention. We can oer a few pieces of advice regarding their
evaluation. One is that the independence of the research is key; the research team
should be independent of the funder (as our own research is). This helps ensure
that all the ndings will be published, irrespective of whether they are positive or
negative. The second piece of advice regards the risks of co-production of research,
an increasingly common approach. Co-production makes sense in many contexts
(for example, co-production with patients), but in others – in particular, in research
on commercial determinants, and public-private partnerships more generally – co-
production may carry risks. For example, it may compromise the independence of
the research, if it involves co-production with certain stakeholders (such as policy-
makers, or businesses). Formative evaluations in particular may make it dicult for
the researchers to maintain independence.

143
Public health and the food and drinks industry: The governance and ethics of interaction COMMENTARY 4
Researchers should also be very cautious about the governance of the research – in
particular, the membership of steering groups and advisory groups, and their terms
of reference. These groups, and the terms of reference, should not be in a position
to interfere with the ability of the researchers to choose the most scientically
appropriate methods, to identify the most relevant public health questions and
outcomes, and to publish all the ndings. (We emphasise that we have not had
these problems in our own research.)
One nal piece of advice is that researchers should not assume that their ndings
will be welcomed even by academic colleagues. Research on complex issues may
often involve mixed-methods analyses, where the researcher is not in control of the
delivery of the intervention. Randomised controlled trials are unlikely to be feasible.
Evaluations which conclude that an intervention is ‘eective’ or ‘ineective’ may
therefore be impossible – particularly where any outcomes cannot be condently
attributed to the intervention. One may therefore have to invest time in persuading
academic colleagues that a good process evaluation is as scientically rigorous, and
more valuable to decision-makers, than a weak or meaningless outcome evaluation.
Conclusion
The implications of the experiences outlined in these case studies are rst, as
highlighted by them all, that we cannot aord to invest in ineective approaches to
public health in light of the growing burden of non-communicable diseases. Second,
there is a need to renew clarity of leadership in public health, emphasising legitimacy
(asking the question of whether this actor / partner has a clear and primary mandate
for public health), accountability, transparency and eectiveness of interventions.
Third, the public has an important role to play: the need for greater public scrutiny
of such partnerships is a key implication of Case 2, the case study about sugar-
sweetened beverage taxation in Chile, an implication which is highly relevant to
other commodities, and other countries. Finally, and perhaps most important of all,
is the implication that the public health community needs to be far more uent in
the language and practice of identifying and managing conicts of interest, because
even in very transparent dealings, as with Case 3 from Fiji, without early mitigation of
conicts, industry interests can undermine public health goals.

144
Public health and the food and drinks industry: The governance and ethics of interactionCOMMENTARY 4
Declarations of interests
Cecile Knai
None declared.
Mark Petticrew
None declared.
References
Bartlett O, Garde A (2015). The EU Platform and the EU Forum: new modes of governance or a smokescreen for the promotion of
conflicts of interest? In: Alemanno A, Garde A (eds).
Regulating Lifestyle Risks: The EU, Alcohol, Tobacco and Unhealthy Diets
.
Cambridge: Cambridge University Press.
Downs SM, Thow AM, Leeder SR (2013). The effectiveness of policies for reducing dietary trans fat: a systematic review of the
evidence.
Bulletin of the World Health Organization
, 91 (4): 262-269h.
Durand MA, Petticrew M, Goulding L, et al (2015). An evaluation of the Public Health Responsibility Deal: Informants’ experiences
and views of the development, implementation and achievements of a pledge-based, public-private partnership to improve
population health in England.
Health Policy
, 119 (11): 1506-14.
Galea G, McKee M (2014). Public-private partnerships with large corporations: setting the ground rules for better health.
Health
Policy
, 115 (2-3): 138-40.
Hendry VL, Almíron-Roig E, Monsivais P, et al (2015). Impact of regulatory interventions to reduce intake of artificial trans-fatty
acids: a systematic review.
American Journal of Public Health
, 105 (3): e32-e42.
Huizinga O, Kruse M (2016). Food industry self-regulation scheme ‘EU Pledge’ cannot prevent the marketing of unhealthy foods to
children.
Obesity Medicine
, 1: 24-28.
Jensen JD, Ronit K (2015). The EU pledge for responsible marketing of food and beverages to children: implementation in food
companies.
European Journal of Clinical Nutrition
, 69 (8): 896-901.
Knai C, Gilmore A, Lock K, et al (2010). Public health research funding: independence is important.
The Lancet,
376 (9735): 75-
77.
Knai C, Petticrew M, Durand MA, et al (2015a). Has a public-private partnership resulted in action on healthier diets in England?
An analysis of the Public Health Responsibility Deal food pledges.
Food Policy
, 54: 1-10.
Knai C, Petticrew M, Scott C, et al (2015b). Getting England to be more physically active: are the Public Health Responsibility
Deal’s physical activity pledges the answer?
International Journal of Behavioral Nutrition and Physical Activity,
12: 107.
Knai C, Petticrew M, Durand MA, et al (2015c). Are the Public Health Responsibility Deal alcohol pledges likely to improve public
health? An evidence synthesis.
Addiction
, 110 (8): 1232-46.
Knai C, Petticrew M, Durand MA, et al (2015d). The Public Health Responsibility Deal: has a public-private partnership brought
about action on alcohol reduction?
Addiction
, 110 (8): 1217-25.
Knai C, Scott C, D’Souza P, et al (2016). The Public Health Responsibility Deal: making the workplace healthier?
Journal of Public
Health
(Oxf), 39(2): 373-86.
Knai C, James L, Petticrew M, et al (2017). An evaluation of a public-private partnership to reduce artificial trans fatty acids in
England, 2011-16.
European Journal of Public Health
, 27 (4): 605-08. doi: 10.1093/eurpub/ckx002
Kunkel DL, Castonguay JS, Filer CR (2015). Evaluating industry self-regulation of food marketing to children.
American Journal of
Preventive Medicine
, 49 (2): 181-87.
Noel JK, Babor TF, Robaina K (2017). Industry self-regulation of alcohol marketing: a systematic review of content and exposure
research.
Addiction
, 112 (1): 28-50.
Petticrew M, Douglas N, Knai C, et al (2016). Health information on alcoholic beverage containers: has the alcohol industry’s
pledge in England to improve labelling been met?
Addiction
, 111 (1): 51-55.
Potvin Kent M, Wanless A (2014). The influence of the Children’s Food and Beverage Advertising Initiative: change in children’s
exposure to food advertising on television in Canada between 2006-2009.
International Journal of Obesity,
38 (4): 558-62.
Potvin Kent ML, Dubois ML, Wanless A (2011). Self-regulation by industry of food marketing is having little impact during
children’s preferred television.
International Journal of Pediatric Obesity,
6 (5-6): 401-08.
Ronit K, Jensen JD (2014). Obesity and industry self-regulation of food and beverage marketing: a literature review.
European
Journal of Clinical Nutrition
, 68 (7): 753-59.

145
Public health and the food and drinks industry: The governance and ethics of interaction CONCLUSIONS
Authors
Jeff Collin
University of
Edinburgh
Rima Afifi
American University
of Beirut
Fabio Gomes
Pan American Health
Organization
The cases outlined in this Casebook make an important contribution to increasing
understanding of the challenges and opportunities associated with partnership
and multi-stakeholder approaches to addressing the global burden of non-
communicable diseases (NCDs). In examining the lessons learned from multiple
initiatives across diverse geographical and policy contexts, they begin to address a
major gap in health policy research and practice – a gap that is as surprising as it is
signicant, given the current prominence of such multi-stakeholder collaborations.
Partnerships across governments, civil society actors and the commercial sector
are currently being promoted as a key mechanism for achieving positive health
outcomes. The Sustainable Development Goals (SDGs) position partnership as
a core principle of good governance for sustainable development, with goal 17
committing to encouraging “multi-stakeholder partnerships that mobilise and
share knowledge, expertise, technology and nancial resources”, and to “eective
public, public-private and civil society partnerships, building on the experience
and resourcing strategies of partnerships” (United Nations, 2016). The emphasis
on building and broadening collaborative approaches is similarly evident within the
World Health Organization (WHO), notably in the context of the protracted and
contentious reforms associated with the Framework for Engagement with Non-
State Actors (Buse and Hawkes, 2016). A Global Co-ordination Mechanism for
the Prevention and Control of NCDs has also been developed, with a remit “to
facilitate and enhance coordination of activities, multi-stakeholder engagement and
action across sectors at the local, national, regional and global levels” (World Health
Organization, 2014).
Governance mechanisms largely neglect conflicts of interest
In the context of global encouragement of multi-stakeholder partnerships, perhaps
the single most striking feature of the collection of cases presented here is the
frequency with which conicts of interest are cited as a principal challenge to the
viability or appropriateness of these approaches. Cases 1 and 7 from Mexico
highlight the centrality of conicts of interest to the development of obesity policy,
and raise concerns about multi-stakeholder processes providing privileged access
for commercial sector actors over public health and civil society voices. In the cases
from Brazil and Chile (Cases 2, 4 and 6), conicts of interest are presented as an
impediment to the development of eective policy, and Case 9 from Spain highlights
the scope for partnership to serve to legitimise the positions and practices of the
alcohol industry.
The cases presented here also indicate that such conicts of interest are often
neglected in governance mechanisms, and that existing practices for their
Conclusions
CONCLUSIONS

146
Public health and the food and drinks industry: The governance and ethics of interactionCONCLUSIONS
management tend to be inadequate. The reections of a former Minister of Health
in Fiji (see Case 3) are invaluable, both in noting the neglect of ethical issues when
including the sugar-sweetened beverage (SSB) industry in the development of NCD
policy, and in highlighting the technical challenge to government ocials in managing
such complex interactions. In the context of global governance, the case study of
opportunistic engagement by drinks manufacturers in the Global Health Council
(Case 10) similarly highlights the complexity of managing conicts of interest in
partnerships involving civil society.
Learning from past experience with tobacco control
This concern with governance is reected in cases where authors highlight
opportunities to learn from the experience of colleagues in tobacco control. This
includes drawing parallels between the conduct and strategies of food and drinks
manufacturers in Chile and Mexico and more extensively documented analyses of
the corporate political activity of tobacco companies, and also pointing towards
tobacco control’s more developed policies with respect to preventing industry
interference in policy-making (Framework Convention Alliance, 2017). The cases
suggest a need to develop comparable oversight mechanisms and policies for
managing any interactions with the alcohol and food and beverages industries.
Diversity of experiences of public-private interactions
It is also important to recognise the diversity of experiences and perspectives that
exist across the Casebook. The majority of case studies are clearly very cautious
about the scope for collaboration with producers of unhealthy commodities and
point to clear struggles in ensuring public health as the primary aim in those
partnerships. In contrast, a study by leading participants within the EPODE
International Network (Case 12) highlights the continuing relevance to current
practice of the claim that “an enlightened private industry partner can contribute in
a positive manner without conicts”. The prominence of the EPODE network, and
its origins as a private initiative by transnational producers of ultra-processed foods,
illustrate the ongoing role of the food and beverage industry in actively shaping the
terms of discourse regarding collaborative approaches and conicts of interest.
Working with commercial sector actors
Among the most complex and thought-provoking cases presented in the Casebook
is Case 8 from colleagues in Guatemala. In developing images to test responses to
front-of-package labels on food products, researchers entered into a partnership
with a design company which had extensive experience of working with the

147
Public health and the food and drinks industry: The governance and ethics of interaction CONCLUSIONS
beverage industry. This constitutes a recognition of the relevant expertise that
commercial sector actors can bring to specic public health initiatives, indicates
a willingness to proactively engage with ethical and policy issues associated with
conict of interest, and acknowledges the heightened pressures towards partnership
in resource-limited settings. Their willingness to embrace the complexity, and to
consider how to deal with conicts of interest beyond producers of unhealthy
commodities, points towards the need for much more sensitive tools to support
policy-makers, public ocials, researchers and civil society organisations.
Skills and tools needed to support public health actors
The need to better support public health actors in deciding whether or how
to engage in multi-stakeholder partnerships is powerfully articulated in the
Commentaries (see page 132). Collectively, these further the sense, conveyed by
the cases, of problems being widely shared and arguably being global, albeit often
experienced in distinctive ways across dierent contexts. Hence perspectives from
both the UK and in the Western Pacic region call for health actors to be equipped
with new skills to increase capacity to navigate this contentious terrain, while
colleagues from the Americas seek improved denition of and dierentiation among
public and private actors, interests and roles. The relevance of regional contexts in
compounding global challenges is most powerfully evident in the Caribbean; here
economic vulnerability, social and cultural context and state capacity all emerge as
signicant factors for developing locally relevant solutions to global problems.
Summary
In summary, the cases presented in this Casebook highlight the following key
challenges associated with partnership and multi-stakeholder approaches to
reducing the global burden of NCDs.
• The cases collectively illustrate a striking contrast between the broad political
commitments to collaboration and the limited evidence base for the eectiveness
of partnership approaches to improving nutrition.
• They demonstrate the ongoing tendency of partnerships to fail to establish
adequate governance mechanisms that could promote eectiveness, including
with reference to monitoring, enforcement and sanctions for non-compliance.
• The diculty of adequately identifying and managing conicts, and the insuciency
of existing tools, reinforce a tendency to tacitly assume scope for convergence of
interest across sectors and stakeholders.

148
Public health and the food and drinks industry: The governance and ethics of interactionCONCLUSIONS
•‘Interests’and‘industries’arenotyetsucientlywelldenedtosupportpolicy-
makersandadvocatesinidentifyingpotentiallyusefulpartnersorindeveloping
appropriatetermsofengagementinpolicyorresearch.
Recommendations
TheCasebookmarksasignicantstepforwardinarticulatingsuchchallengesand
alsoinguidingthinkingabouthowtorespondtoemergentopportunitieswithin
globalhealth.Whiletheindividualcasesprovidealternativescenarioswhichreect
onhowthingsmighthavebeendonedierently,theCasebookidentiesthree
overarchingrecommendationsforpublichealthactors:
1 TheSustainableDevelopmentGoalsincludecommitmentsbothtoreducing
mortalityfromNCDsandtoensuringpolicycoherenceforsustainable
development.Thiscreatesscopetore-thinkaspectsofthepartnershipparadigm
insuchcontexts,andtodevelopmoreconsistentapproachestointeractionswith
tobacco,alcoholandultra-processedfoodindustriesinaddressingthecommercial
determinantsofhealth(CollinandCasswell,2016).
2 Theimperativetoengagemoreeectivelywithquestionsofconictsofinterest
isreectedinWHO’scommitmenttocreateriskassessmentandmanagement
toolstosupportmemberstatesindevelopingeectivenutritionpolicies(World
HealthOrganization,2016).Comparableresourcesarealsoneededforcivilsociety
organisationsandforresearchinstitutions.
3 Inaddition,furtherresearchisrequiredtomonitorandevaluateanyunintended
consequencesarisingfromthesemulti-stakeholderpartnerships.Suchinitiatives
mustbeparticularlyresponsivetothediverseneedsofpublicocialsandhealth
actorsinlow-andmiddle-incomecountrieswhereresourceconstraintsandpower
dierentialsbetweenprivateandpublicactorsmaypresentadditionalchallenges.
TheCasebookprovidesthemostextensiveandthoughtfuldocumentationofsuch
needstodate,andhighlightstheneedforresearchersandfunderstosupportnew
inter-disciplinaryapproachestoaddressingapressingchallengeinglobalhealth
governance.
149
Public health and the food and drinks industry: The governance and ethics of interaction CONCLUSIONS
Declarations of interests
Rima Afifi
None declared.
Jeff Collin
None declared.
Fabio Gomes
None declared.
References
Buse K, Hawkes S (2016). Sitting on the FENSA: WHO engagement with industry.
The Lancet,
388 (10043): 446.
Collin J, Casswell S (2016). Alcohol and the sustainable development goals.
The Lancet,
387 (10038): 2582.
Framework Convention Alliance (2017). Article 5.3, Framework Convention on Tobacco Control – Tobacco Industry Interference.
http://www.fctc.org/media-and-publications/media-releases-blog-list-view-of-all-313/industry-interference/718-article-53-
framework-convention-on-tobacco-control-tobacco-industry-interference [Accessed 4 November 2017.]
United Nations (2016).
Sustainable Development Goals.
http://www.un.org/sustainabledevelopment/sustainable-development-goals/
World Health Organization (2014).
Prevention and Control of Noncommunicable Diseases: Terms of Reference for the Global
Coordination Mechanism on the Prevention and Control of Noncommunicable Diseases. Report by the Director-General
.
A67/14 Add 1. 8 May 2014. http://apps.who.int/gb/ebwha/pdf_files/WHA67/A67_14Add1-en.pdf?ua=1
World Health Organization (2016).
Addressing and Managing Conflicts of Interest in the Planning and Delivery of Nutrition
Programmes at Country Level. Report of a Technical Consultation Convened in Geneva, Switzerland, on 8-9 October 2015
.
Geneva: World Health Organization. http://www.who.int/nutrition/publications/COI-report/en/

Public health and the food and drinks industry:
The governance and ethics of interaction. Lessons from research, policy and practice
ISBN E-version: 978-1-874279-16-7